

Neuroimaging features of genetic syndromes associated with CNS overgrowth
- PMID: 36207456
- PMCID: PMC9701655
- DOI: 10.1007/s00247-022-05408-5
Neuroimaging features of genetic syndromes associated with CNS overgrowth
Abstract
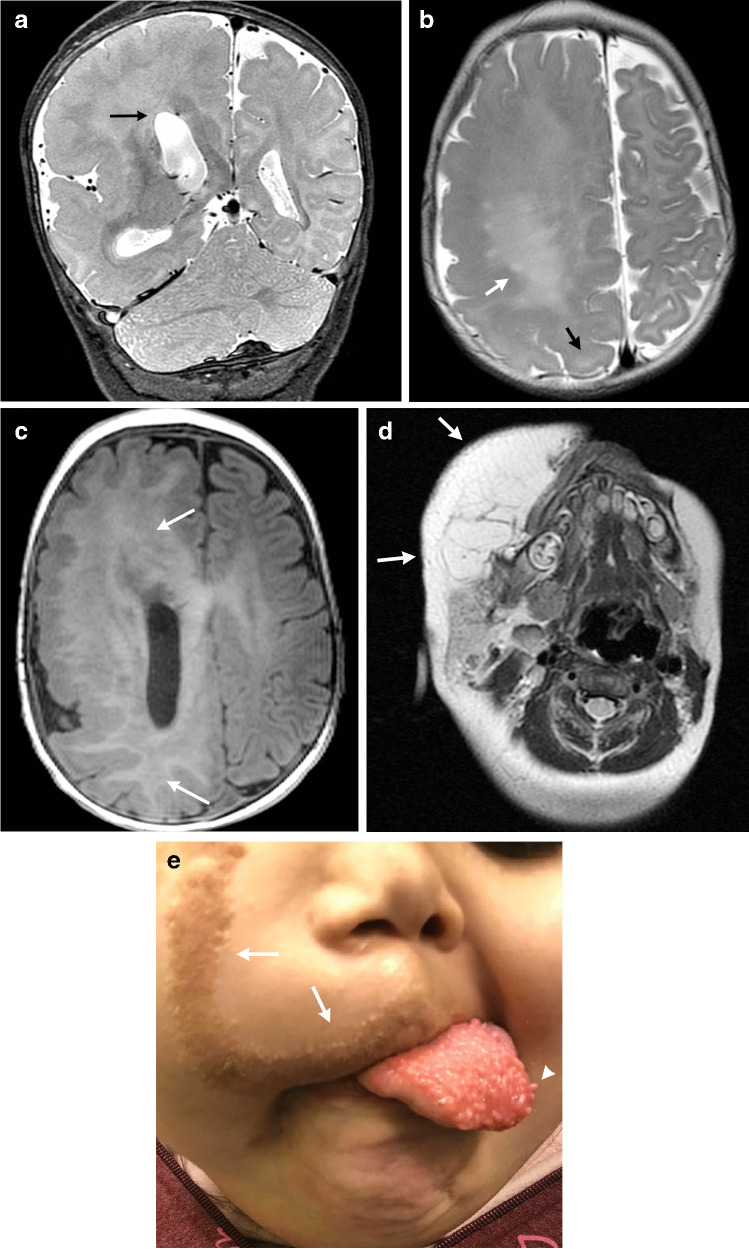
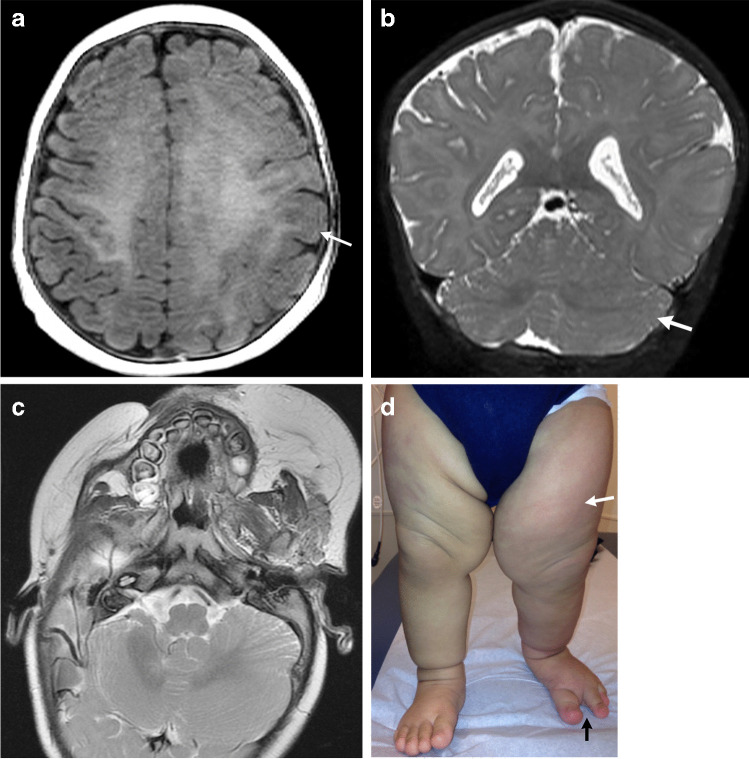
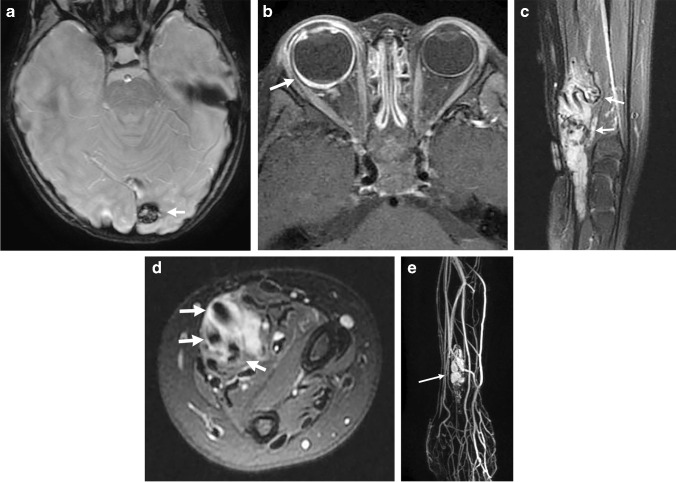
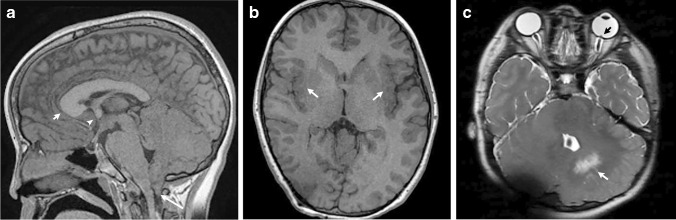
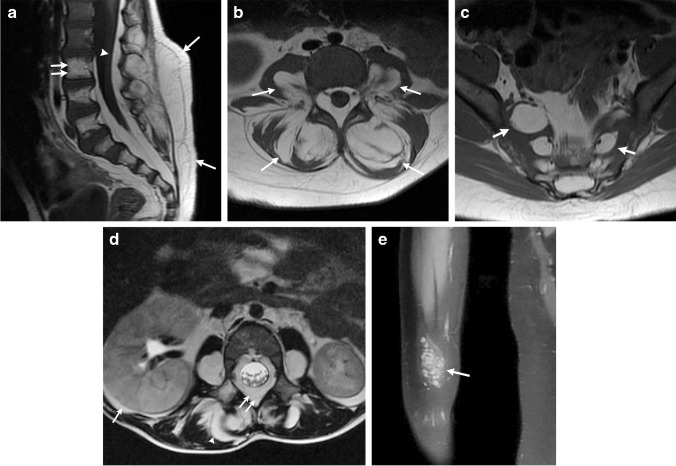
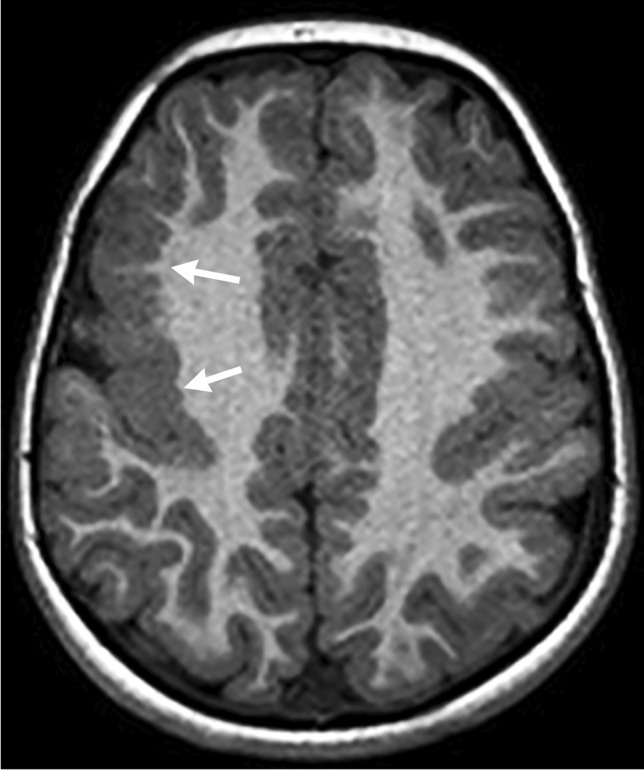
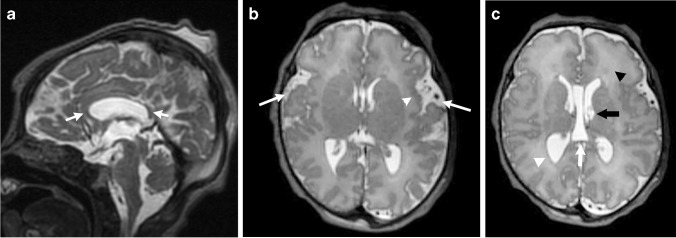
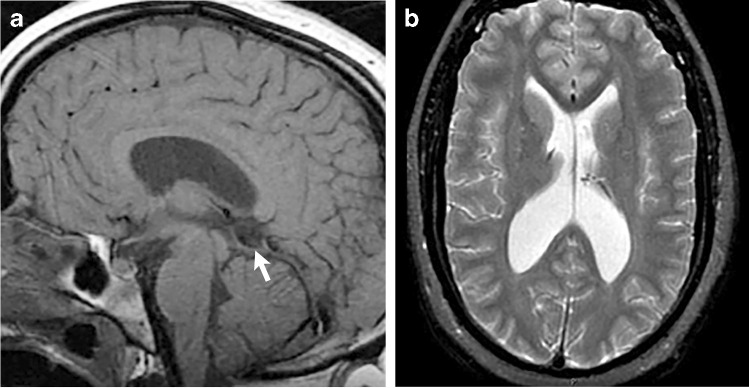
Overgrowth syndromes can manifest with enlargement of the brain and other body parts and are associated with malignancy. Much of the current literature focuses on the imaging findings of the somatic overgrowth, while there is relatively little describing the overgrowth of the central nervous system. In this pictorial essay, we discuss common syndromes with central nervous system overgrowth, highlight key imaging features, and review the underlying genetics, including the PI3K-AKT-mTOR pathway as well as other syndromes from various genes.
Keywords: Central nervous system; Children; Hemimegalencephaly; Magnetic resonance imaging; Overgrowth syndromes; PIK3CA; Vascular malformations.
© 2022. The Author(s).
Conflict of interest statement
None
Figures



References
-
- Mirzaa G, Graham JM, Jr, Keppler-Noreuil K, et al. PIK3CA-related overgrowth spectrum. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews. Seattle: University of Washington; 2013.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
