

Strategies for Using Antigen Rapid Diagnostic Tests to Reduce Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 in Low- and Middle-Income Countries: A Mathematical Modelling Study Applied to Zambia
- PMID: 36208211
- PMCID: PMC9619661
- DOI: 10.1093/cid/ciac814
Strategies for Using Antigen Rapid Diagnostic Tests to Reduce Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 in Low- and Middle-Income Countries: A Mathematical Modelling Study Applied to Zambia
Abstract
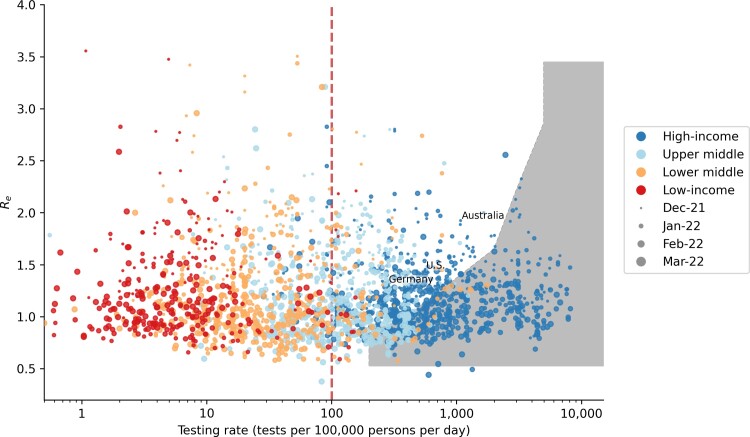
Background: Increasing the availability of antigen rapid diagnostic tests (Ag-RDTs) in low- and middle-income countries (LMICs) is key to alleviating global SARS-CoV-2 testing inequity (median testing rate in December 2021-March 2022 when the Omicron variant was spreading in multiple countries: high-income countries = 600 tests/100 000 people/day; LMICs = 14 tests/100 000 people/day). However, target testing levels and effectiveness of asymptomatic community screening to impact SARS-CoV-2 transmission in LMICs are unclear.
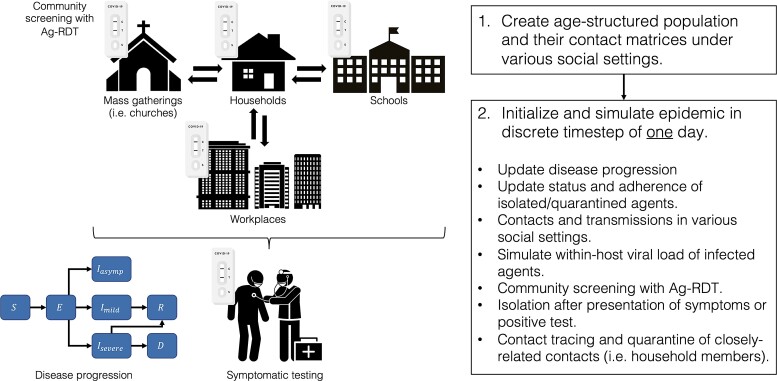
Methods: We used Propelling Action for Testing and Treating (PATAT), an LMIC-focused agent-based model to simulate coronavirus disease 2019 (COVID-19) epidemics, varying the amount of Ag-RDTs available for symptomatic testing at healthcare facilities and asymptomatic community testing in different social settings. We assumed that testing was a function of access to healthcare facilities and availability of Ag-RDTs. We explicitly modelled symptomatic testing demand from individuals without SARS-CoV-2 and measured impact based on the number of infections averted due to test-and-isolate.
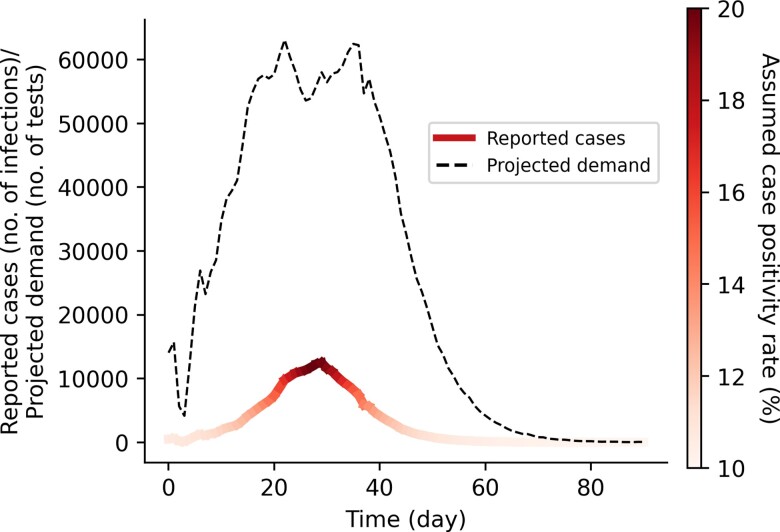
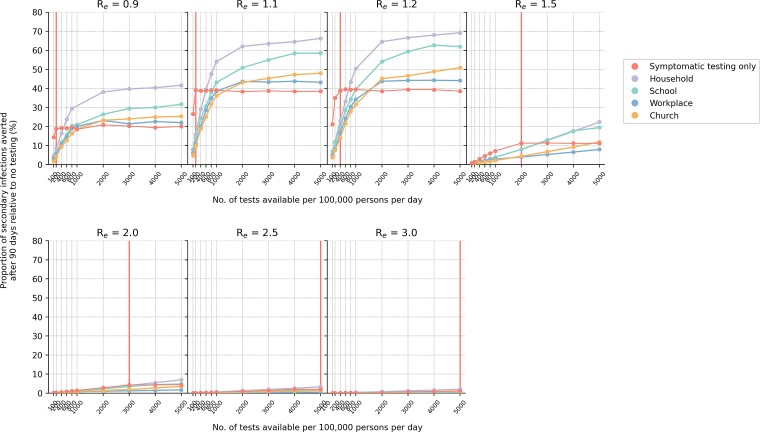
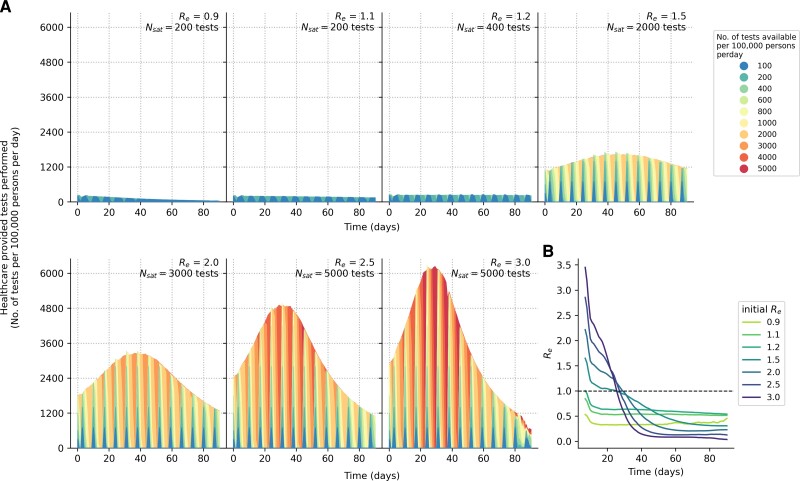
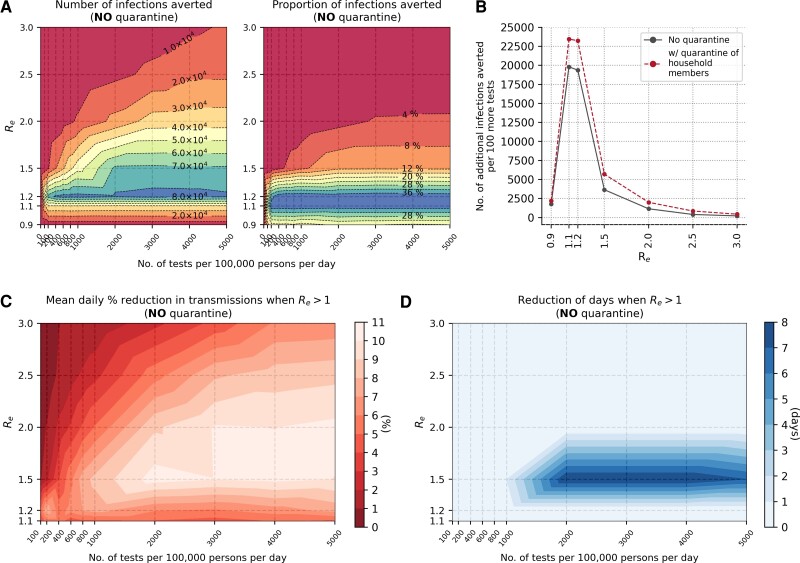
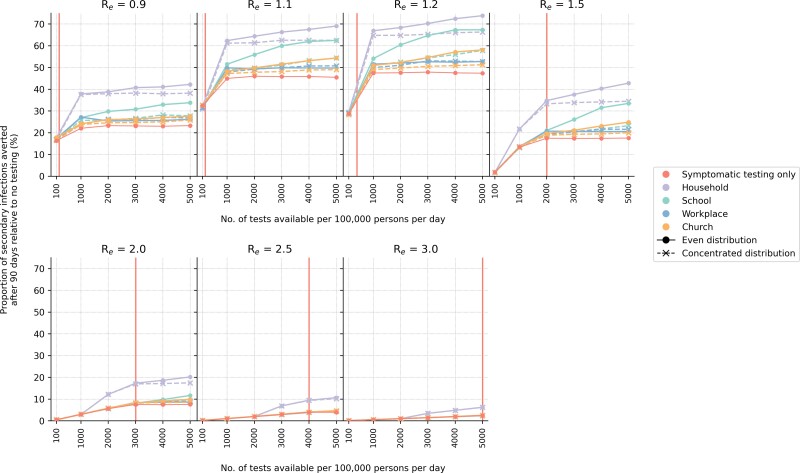
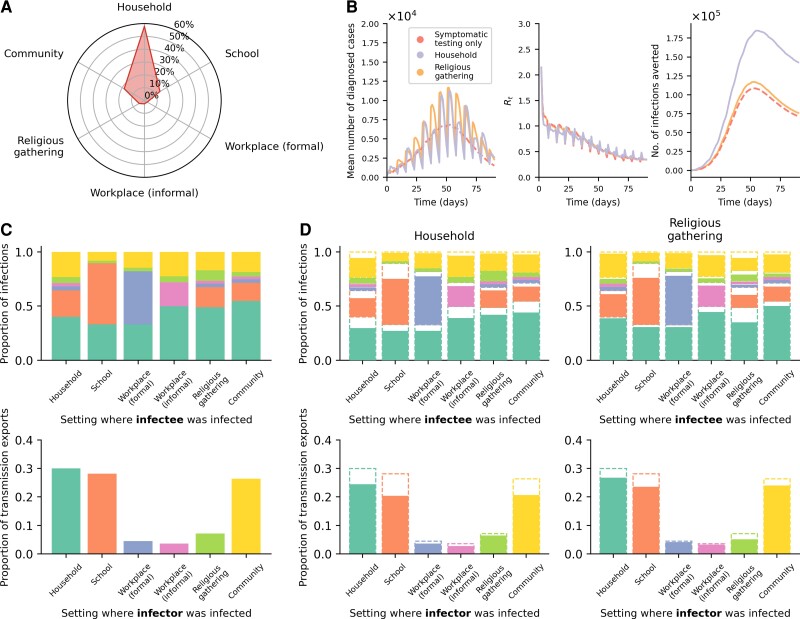
Results: Testing symptomatic individuals yields greater benefits than any asymptomatic community testing strategy until most symptomatic individuals who sought testing have been tested. Meeting symptomatic testing demand likely requires at least 200-400 tests/100 000 people/day, on average, as symptomatic testing demand is highly influenced by individuals without SARS-CoV-2. After symptomatic testing demand is satisfied, excess tests to proactively screen for asymptomatic infections among household members yield the largest additional infections averted.
Conclusions: Testing strategies aimed at reducing transmission should prioritize symptomatic testing and incentivizing test-positive individuals to adhere to isolation to maximize effectiveness.
Keywords: COVID-19; SARS-CoV-2; diagnostic testing; low- and middle-income countries.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. J. A. S., A. T., N. H., and E. H. are employed by Foundation for Innovative New Diagnostics (FIND), the global alliance for diagnostics. A. X. H. reports consulting fees from Boston University (paid to author). The other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
