

Prognostic value of plasma circulating tumor DNA fraction across four common cancer types: a real-world outcomes study
- PMID: 36208697
- PMCID: PMC9805517
- DOI: 10.1016/j.annonc.2022.09.163
Prognostic value of plasma circulating tumor DNA fraction across four common cancer types: a real-world outcomes study
Abstract
Background: Genomic analysis of circulating tumor DNA (ctDNA) is increasingly incorporated into the clinical management of patients with advanced cancer. Beyond tumor profiling, ctDNA analysis also can enable calculation of circulating tumor fraction (TF), which has previously been found to be prognostic. While most prognostic models in metastatic cancer are tumor type specific and require significant patient-level data, quantification of TF in ctDNA has the potential to serve as a pragmatic, tumor-agnostic prognostic tool.
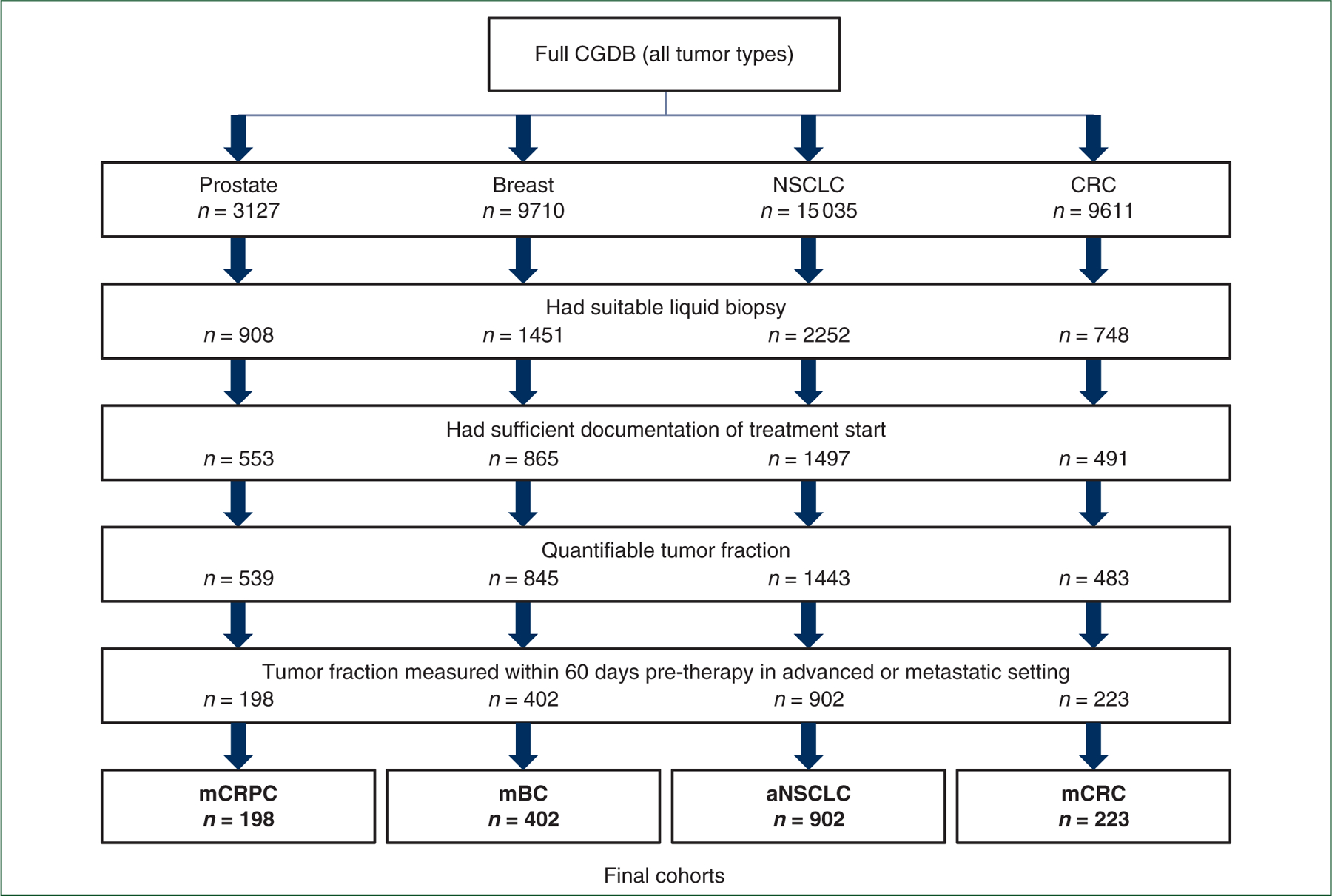
Patients and methods: This study utilized a cohort of patients in a nationwide de-identified clinico-genomic database with metastatic castration-resistant prostate cancer (mCRPC), metastatic breast cancer (mBC), advanced non-small-cell lung cancer (aNSCLC), or metastatic colorectal cancer (mCRC) undergoing liquid biopsy testing as part of routine care. TF was calculated based on single-nucleotide polymorphism aneuploidy across the genome. Clinical, disease, laboratory, and treatment data were captured from the electronic health record. Overall survival (OS) was evaluated by TF level while controlling for relevant covariables.
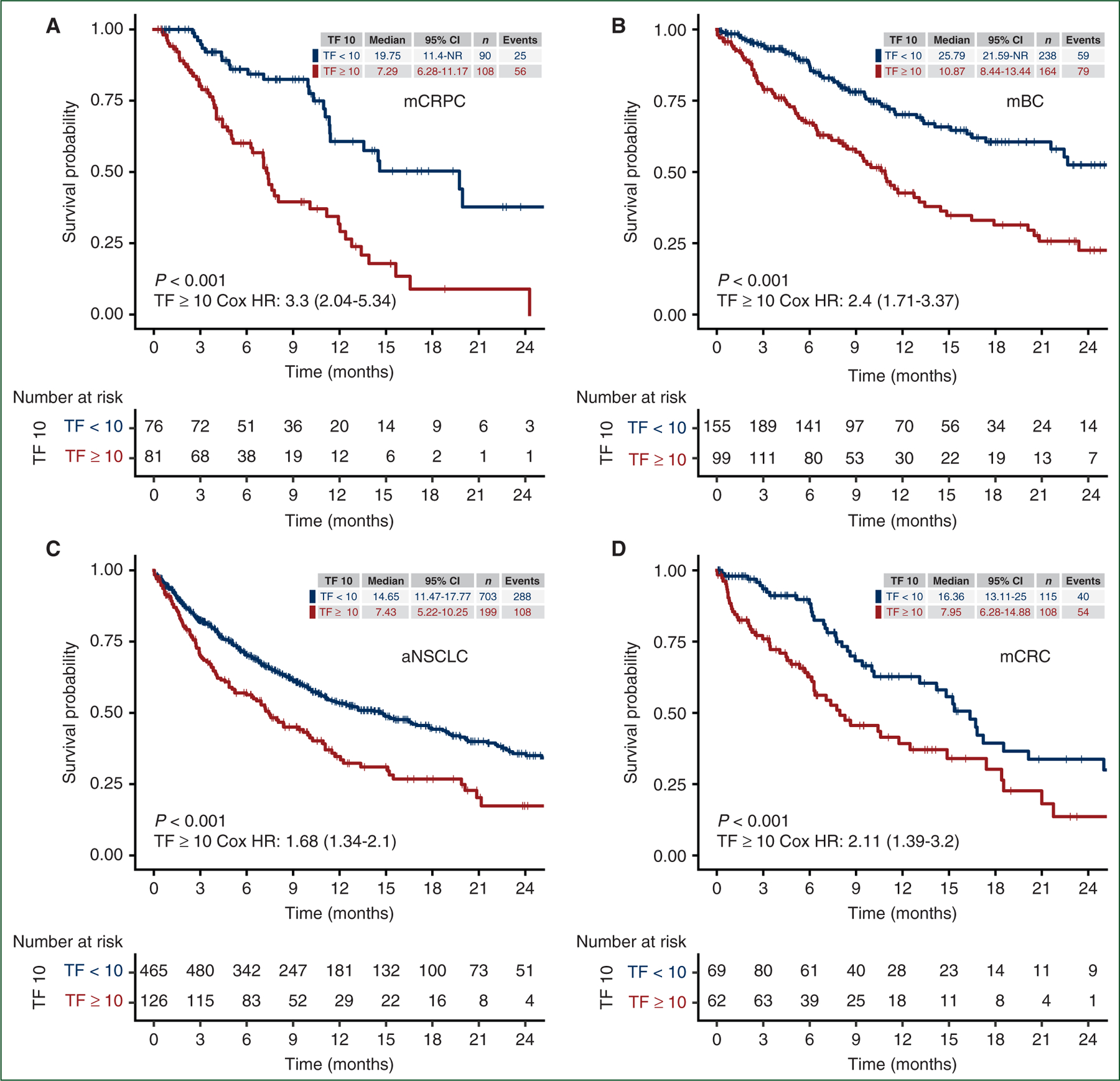
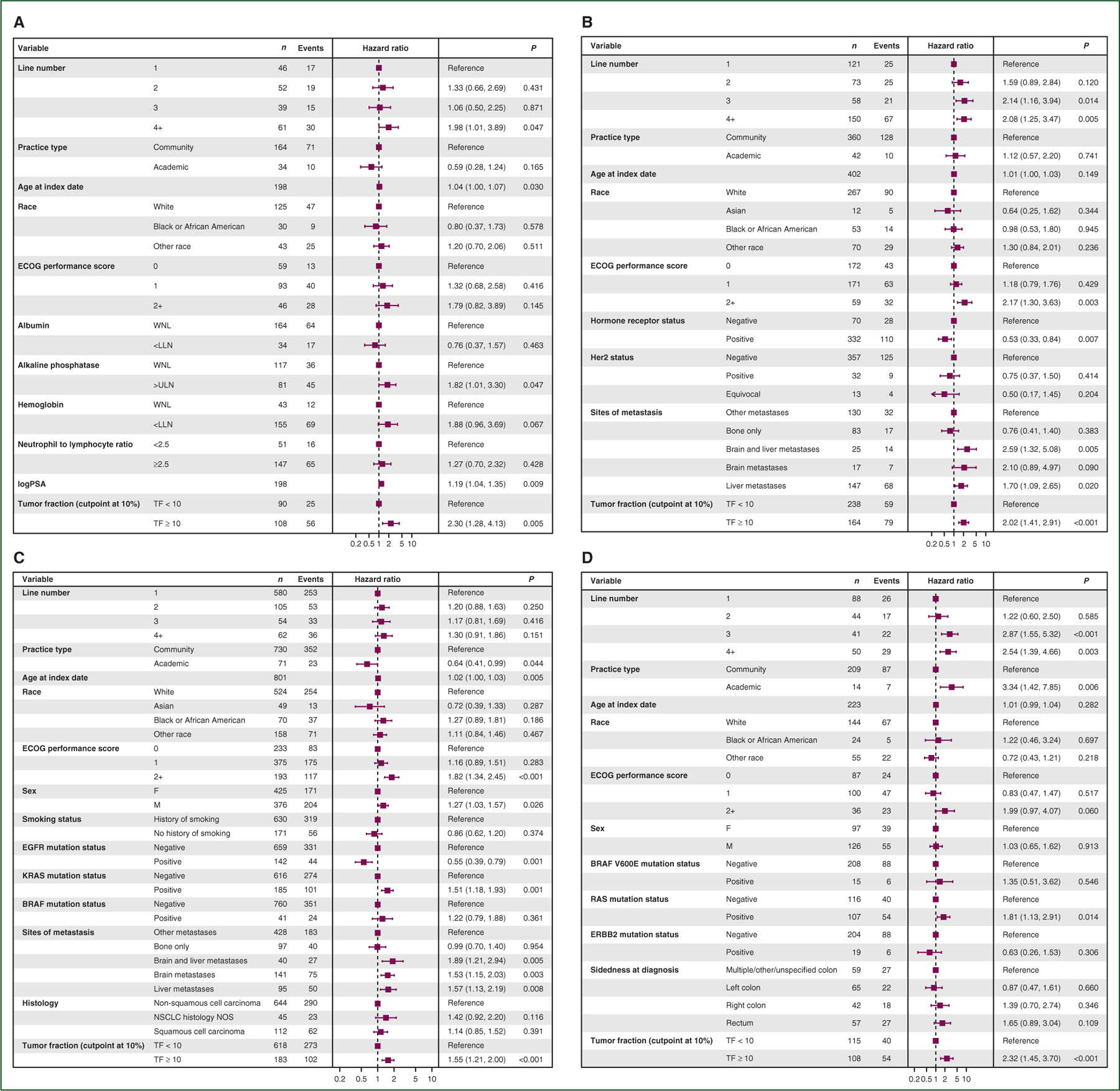
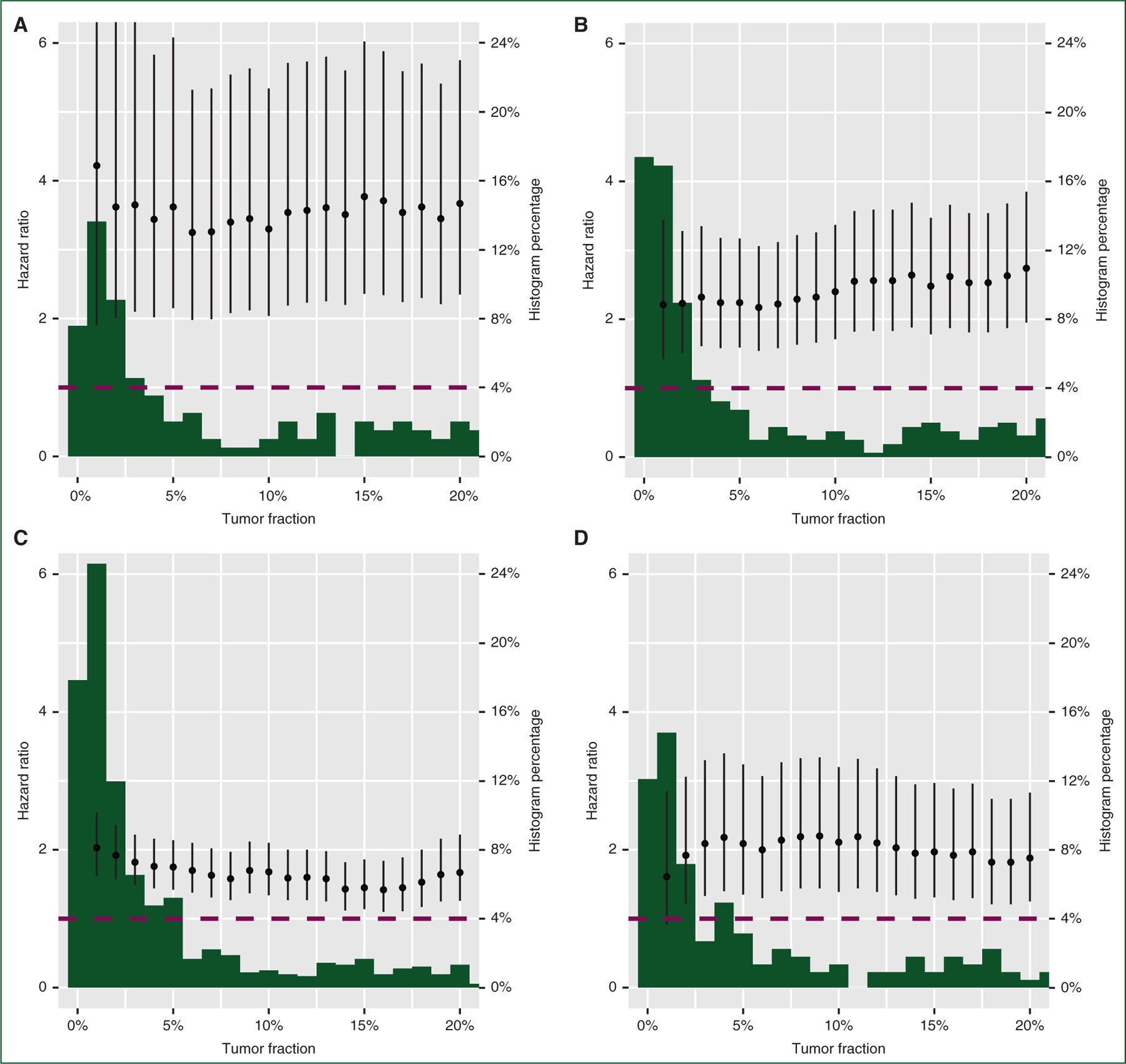
Results: A total of 1725 patients were included: 198 mCRPC, 402 mBC, 902 aNSCLC, and 223 mCRC. TF ≥10% was highly correlated with OS in univariable analyses for all cancer types: mCRPC [hazard ratio (HR) 3.3, 95% confidence interval (CI) 2.04-5.34, P < 0.001], mBC (HR 2.4, 95% CI 1.71-3.37, P < 0.001), aNSCLC (HR 1.68, 95% CI 1.34-2.1, P < 0.001), and mCRC (HR 2.11, 95% CI 1.39-3.2, P < 0.001). Multivariable assessments of TF had similar point estimates and CIs, suggesting a consistent and independent association with survival. Exploratory analysis showed that TF remained consistently prognostic across a wide range of cutpoints.
Conclusions: Plasma ctDNA TF is a pragmatic, independent prognostic biomarker across four advanced cancers with potential to guide clinical conversations around expected treatment outcomes. With further prospective validation, ctDNA TF could be incorporated into care paradigms to enable precision escalation and de-escalation of cancer therapy based on patient-level tumor biology.
Keywords: breast cancer; colorectal cancer; non-small-cell lung cancer; prognosis; prostate cancer; tumor fraction.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure Financial disclosures: GL, RWM, ADF, GRO, and RPG are employees of Foundation Medicine, a wholly owned subsidiary of Roche, and have equity interest in Roche. EC and TS are employees of Flatiron Health, a wholly owned subsidiary of Roche, and have equity interest in Roche. DGS has participated on an advisory board with Novartis. ZRR has received consulting fees and institutional funding from AstraZeneca. TMM has participated in an advisory board for Myovant Sciences. FGD has declared no conflicts of interest.
Figures
References
-
- Ignatiadis M, Sledge GW, Jeffrey SS. Liquid biopsy enters the clinic—implementation issues and future challenges. Nat Rev Clin Oncol 2021;18:297–312. - PubMed
-
- Lindsay CR, Blackhall FH, Carmel A, et al. EPAC-lung: pooled analysis of circulating tumour cells in advanced non-small cell lung cancer. Eur J Cancer 2019;117:60–68. - PubMed
-
- Kowalik A, Kowalewska M, Góźdź S. Current approaches for avoiding the limitations of circulating tumor cells detection methods - implications for diagnosis and treatment of patients with solid tumors. Transl Res 2017;185:58–84.e15. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
