

Efficacy and Safety of Filgotinib in Patients with High Risk of Poor Prognosis Who Showed Inadequate Response to MTX: A Post Hoc Analysis of the FINCH 1 Study
- PMID: 36209441
- PMCID: PMC9931960
- DOI: 10.1007/s40744-022-00498-x
Efficacy and Safety of Filgotinib in Patients with High Risk of Poor Prognosis Who Showed Inadequate Response to MTX: A Post Hoc Analysis of the FINCH 1 Study
Erratum in
-
Correction: Efficacy and Safety of Filgotinib in Patients with High Risk of Poor Prognosis Who Showed Inadequate Response to MTX: A Post Hoc Analysis of the FINCH 1 Study.Rheumatol Ther. 2023 Feb;10(1):71-72. doi: 10.1007/s40744-022-00530-0. Rheumatol Ther. 2023. PMID: 36598735 Free PMC article. No abstract available.
Abstract
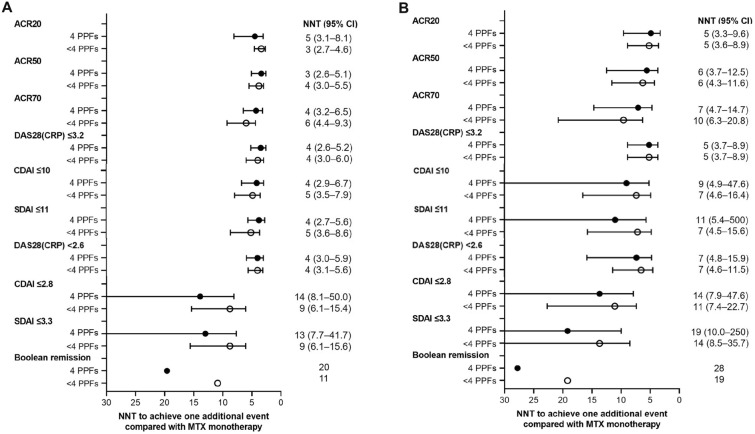
Introduction: This exploratory analysis of FINCH 1 (NCT02889796) examined filgotinib (FIL) efficacy and safety in a subgroup of patients with rheumatoid arthritis (RA) and inadequate response to methotrexate (MTX; MTX-IR) who had four poor prognostic factors (PPFs).
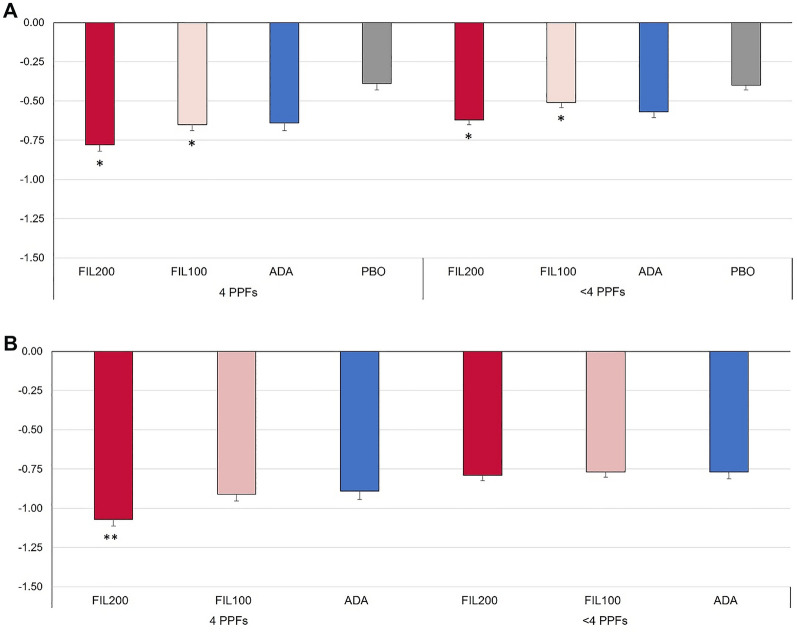
Methods: Patients with MTX-IR received placebo up to week (W)24 or FIL200 mg, FIL100 mg, or adalimumab up to W52; all received MTX. Efficacy and safety data were stratified by four PPFs versus fewer than four PPFs: seropositivity, high-sensitivity C-reactive protein (CRP) ≥ 6 mg/L, Disease Activity Score in 28 joints with CRP > 5.1, and erosions on X-rays.
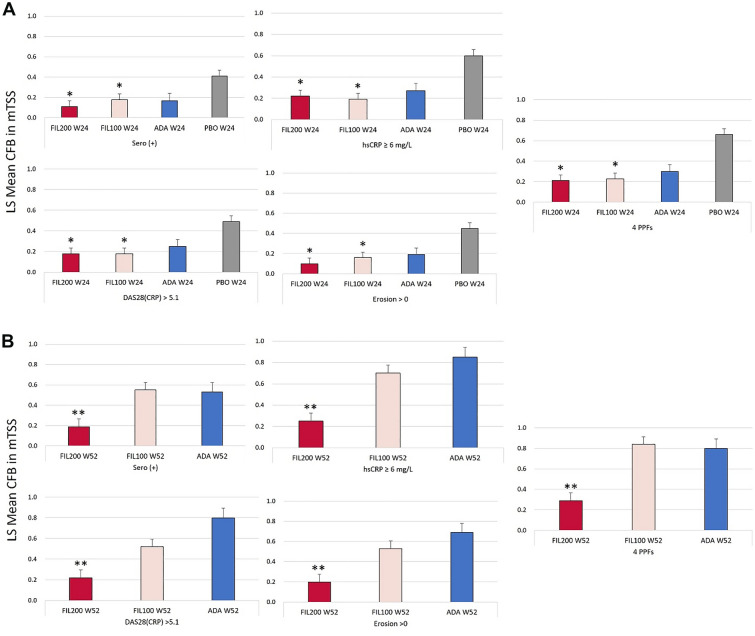
Results: At baseline, 687/1755 patients had four PPFs. At W12, whether with four PPFs or fewer than four PPFs, response rates on all American College of Rheumatology (ACR) measures were significantly greater with FIL200 and FIL100 versus placebo. At W52, FIL200 ACR20/50/70 response rates remained at least numerically higher versus adalimumab in both subgroups. At W52, FIL200 reduced modified total Sharp score (mTSS) change versus adalimumab in patients with four or fewer than four PPFs.
Conclusions: In high-risk (four PPFs) patients with MTX-IR RA, FIL200 and FIL100 showed similar reductions in disease activity versus placebo at W12 as in patients with fewer than four PPFs. mTSS in patients receiving FIL200 changed little from W24 to W52, while that in patients receiving FIL100 progressed comparably to patients who received adalimumab. Tolerability was comparable across treatment arms and subgroups.
Keywords: Adalimumab; Filgotinib; Methotrexate; Poor prognostic factors.
© 2022. The Author(s).
Figures


Similar articles
-
Prevention of Radiographic Progression in Higher-Risk Patients with Rheumatoid Arthritis Using Filgotinib in Phase III Studies: Narrative Review of Post Hoc Analyses.Rheumatol Ther. 2023 Dec;10(6):1399-1415. doi: 10.1007/s40744-023-00590-w. Epub 2023 Sep 5. Rheumatol Ther. 2023. PMID: 37668865 Free PMC article. Review.
-
Benefit of Filgotinib, a JAK1 Preferential Inhibitor, in Rheumatoid Arthritis Patients with Previous Rapid Radiographic Progression: Post Hoc Analysis of Two Trials.Rheumatol Ther. 2023 Feb;10(1):161-185. doi: 10.1007/s40744-022-00503-3. Epub 2022 Nov 3. Rheumatol Ther. 2023. PMID: 36327094 Free PMC article.
-
Efficacy and safety of filgotinib in methotrexate-naive patients with rheumatoid arthritis with poor prognostic factors: post hoc analysis of FINCH 3.RMD Open. 2021 Aug;7(2):e001621. doi: 10.1136/rmdopen-2021-001621. RMD Open. 2021. PMID: 34385364 Free PMC article. Clinical Trial.
-
The impact of filgotinib on patient-reported outcomes and health-related quality of life for patients with active rheumatoid arthritis: a post hoc analysis of Phase 3 studies.Arthritis Res Ther. 2022 Jan 3;24(1):11. doi: 10.1186/s13075-021-02677-7. Arthritis Res Ther. 2022. PMID: 34980223 Free PMC article. Clinical Trial.
-
Filgotinib Radiographic and Clinical Efficacy Versus Other JAK Inhibitors and Adalimumab in Patients With Rheumatoid Arthritis and Inadequate Response to Methotrexate: A Systematic Review and Network Meta-Analysis.Rheumatol Ther. 2025 Jun;12(3):453-468. doi: 10.1007/s40744-025-00757-7. Epub 2025 Apr 10. Rheumatol Ther. 2025. PMID: 40208566 Free PMC article. Review.
Cited by
-
Selectivity, efficacy and safety of JAKinibs: new evidence for a still evolving story.Ann Rheum Dis. 2024 Jan 11;83(2):139-160. doi: 10.1136/ard-2023-223850. Ann Rheum Dis. 2024. PMID: 37923366 Free PMC article. Review.
-
Prevention of Radiographic Progression in Higher-Risk Patients with Rheumatoid Arthritis Using Filgotinib in Phase III Studies: Narrative Review of Post Hoc Analyses.Rheumatol Ther. 2023 Dec;10(6):1399-1415. doi: 10.1007/s40744-023-00590-w. Epub 2023 Sep 5. Rheumatol Ther. 2023. PMID: 37668865 Free PMC article. Review.
-
Long-Term Safety, Efficacy, and Patient-Centered Outcomes of Filgotinib in the Treatment of Rheumatoid Arthritis: Current Perspectives.Patient Prefer Adherence. 2023 Oct 6;17:2499-2516. doi: 10.2147/PPA.S417677. eCollection 2023. Patient Prefer Adherence. 2023. PMID: 37822545 Free PMC article. Review.
-
The Uncoupling of Disease Activity from Joint Structural Progression in Patients with Rheumatoid Arthritis Treated with Filgotinib.Rheumatol Ther. 2025 Feb;12(1):53-66. doi: 10.1007/s40744-024-00725-7. Epub 2024 Nov 26. Rheumatol Ther. 2025. PMID: 39592547 Free PMC article.
References
-
- Smolen JS, Landewe RBM, Bijlsma JWJ, Burmester GR, Dougados M, Kerschbaumer A, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–699. doi: 10.1136/annrheumdis-2019-216655. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
