

Prospective, Multi-Institutional, Real-Time Next-Generation Sequencing of Pancreatic Cyst Fluid Reveals Diverse Genomic Alterations That Improve the Clinical Management of Pancreatic Cysts
- PMID: 36209796
- PMCID: PMC9844531
- DOI: 10.1053/j.gastro.2022.09.028
Prospective, Multi-Institutional, Real-Time Next-Generation Sequencing of Pancreatic Cyst Fluid Reveals Diverse Genomic Alterations That Improve the Clinical Management of Pancreatic Cysts
Abstract
Background & aims: Next-generation sequencing (NGS) of pancreatic cyst fluid is a useful adjunct in the assessment of patients with pancreatic cyst. However, previous studies have been retrospective or single institutional experiences. The aim of this study was to prospectively evaluate NGS on a multi-institutional cohort of patients with pancreatic cyst in real time.
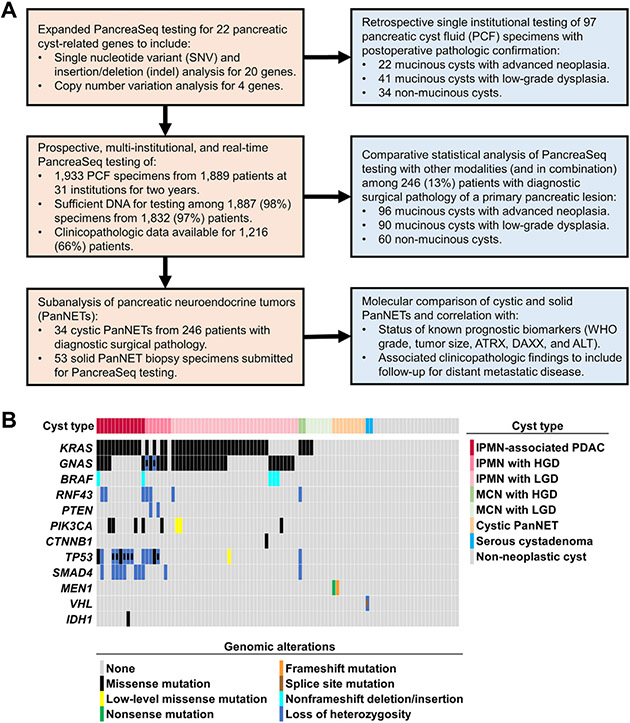
Methods: The performance of a 22-gene NGS panel (PancreaSeq) was first retrospectively confirmed and then within a 2-year timeframe, PancreaSeq testing was prospectively used to evaluate endoscopic ultrasound-guided fine-needle aspiration pancreatic cyst fluid from 31 institutions. PancreaSeq results were correlated with endoscopic ultrasound findings, ancillary studies, current pancreatic cyst guidelines, follow-up, and expanded testing (Oncomine) of postoperative specimens.
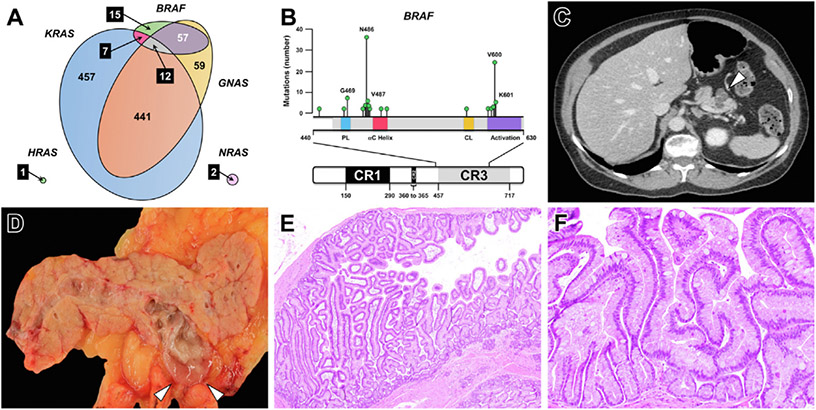
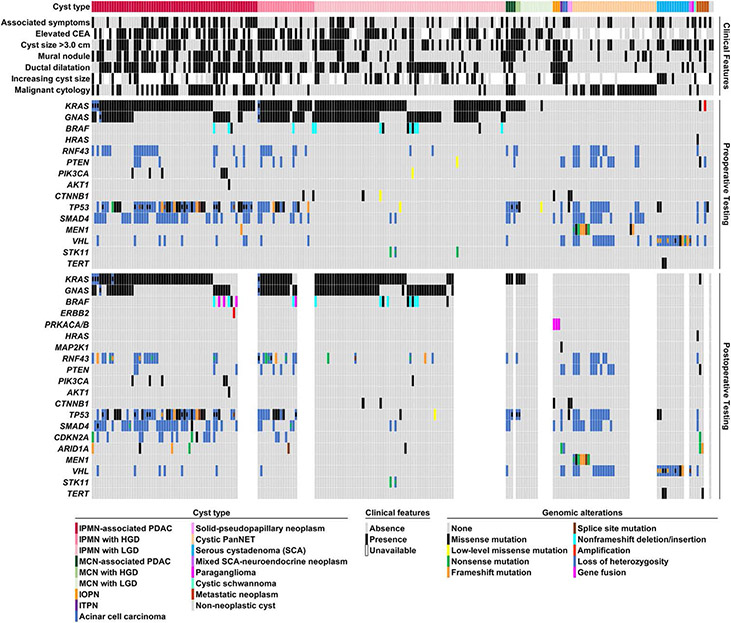
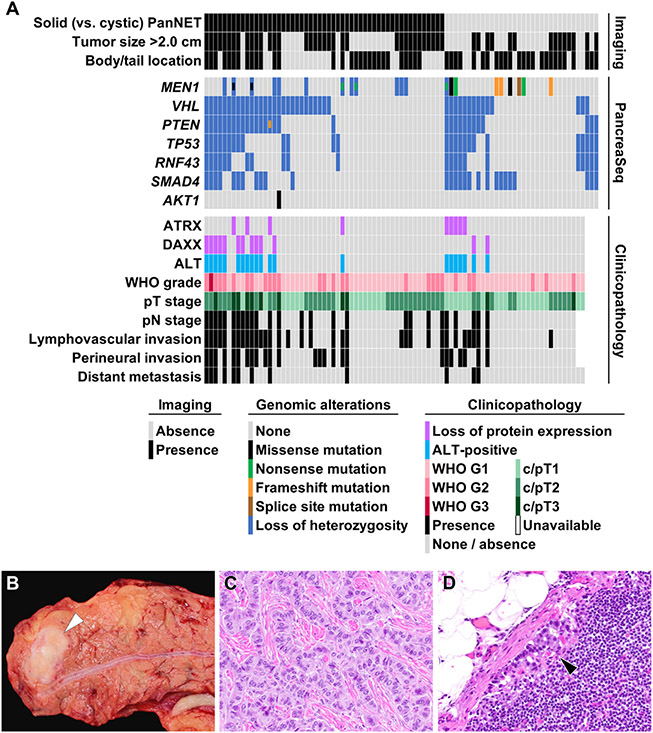
Results: Among 1933 PCs prospectively tested, 1887 (98%) specimens from 1832 patients were satisfactory for PancreaSeq testing. Follow-up was available for 1216 (66%) patients (median, 23 months). Based on 251 (21%) patients with surgical pathology, mitogen-activated protein kinase/GNAS mutations had 90% sensitivity and 100% specificity for a mucinous cyst (positive predictive value [PPV], 100%; negative predictive value [NPV], 77%). On exclusion of low-level variants, the combination of mitogen-activated protein kinase/GNAS and TP53/SMAD4/CTNNB1/mammalian target of rapamycin alterations had 88% sensitivity and 98% specificity for advanced neoplasia (PPV, 97%; NPV, 93%). Inclusion of cytopathologic evaluation to PancreaSeq testing improved the sensitivity to 93% and maintained a high specificity of 95% (PPV, 92%; NPV, 95%). In comparison, other modalities and current pancreatic cyst guidelines, such as the American Gastroenterology Association and International Association of Pancreatology/Fukuoka guidelines, show inferior diagnostic performance. The sensitivities and specificities of VHL and MEN1/loss of heterozygosity alterations were 71% and 100% for serous cystadenomas (PPV, 100%; NPV, 98%), and 68% and 98% for pancreatic neuroendocrine tumors (PPV, 85%; NPV, 95%), respectively. On follow-up, serous cystadenomas with TP53/TERT mutations exhibited interval growth, whereas pancreatic neuroendocrine tumors with loss of heterozygosity of ≥3 genes tended to have distant metastasis. None of the 965 patients who did not undergo surgery developed malignancy. Postoperative Oncomine testing identified mucinous cysts with BRAF fusions and ERBB2 amplification, and advanced neoplasia with CDKN2A alterations.
Conclusions: PancreaSeq was not only sensitive and specific for various pancreatic cyst types and advanced neoplasia arising from mucinous cysts, but also reveals the diversity of genomic alterations seen in pancreatic cysts and their clinical significance.
Keywords: Diagnosis; Early Detection; Pancreas; Pancreatic Cancer; Pancreatic Neoplasm.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
These authors disclose the following: Aatur D. Singhi has received an honorarium from Foundation Medicine, Inc. Ralph H. Hruban has the potential to receive royalty payments from Thrive Earlier Detection for the
Figures
Comment in
-
The "Next Generation" of Pancreatic Cyst Fluid Biomarkers?Gastroenterology. 2023 Jan;164(1):21-23. doi: 10.1053/j.gastro.2022.10.023. Epub 2022 Oct 29. Gastroenterology. 2023. PMID: 36341737 No abstract available.
-
Prospective, Multi-institutional, Real-Time Next-Generation Sequencing of Pancreatic Cyst Fluid.Gastroenterology. 2023 Jul;165(1):304-305. doi: 10.1053/j.gastro.2023.01.009. Epub 2023 Jan 14. Gastroenterology. 2023. PMID: 36646393 No abstract available.
References
-
- Lee KS, Sekhar A, Rofsky NM, et al. Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am J Gastroenterol 2010;105:2079–2084. - PubMed
-
- Marinelli V, Secchettin E, Andrianello S, et al. Psychological distress in patients under surveillance for intraductal papillary mucinous neoplasms of the pancreas: The "Sword of Damocles" effect calls for an integrated medical and psychological approach a prospective analysis. Pancreatology 2020;20:505–510. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
