

The impact of pre-transplant donor specific antibodies on the outcome of kidney transplantation - Data from the Swiss transplant cohort study
- PMID: 36211367
- PMCID: PMC9532952
- DOI: 10.3389/fimmu.2022.1005790
The impact of pre-transplant donor specific antibodies on the outcome of kidney transplantation - Data from the Swiss transplant cohort study
Abstract
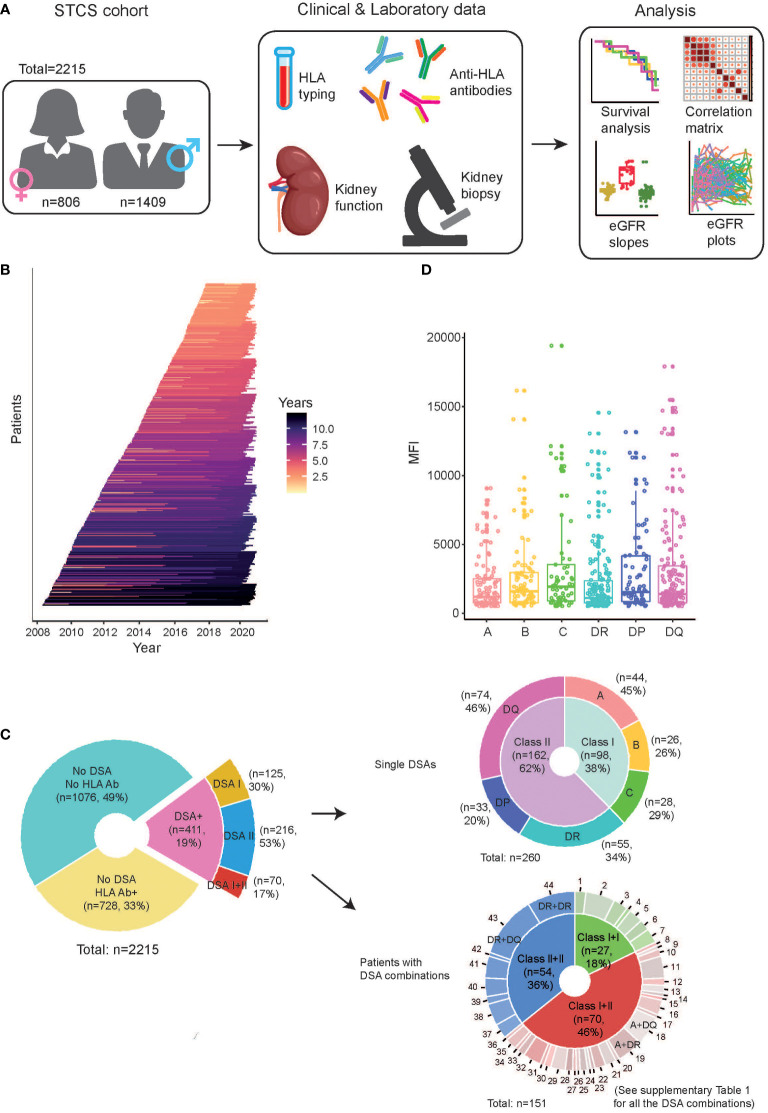
Background: Pre-transplant donor specific antibodies (DSA), directed at non-self human leukocyte antigen (HLA) protein variants present in the donor organ, have been associated with worse outcomes in kidney transplantation. The impact of the mean fluorescence intensity (MFI) and the target HLA antigen of the detected DSA has, however, not been conclusively studied in a large cohort with a complete virtual cross-match (vXM).
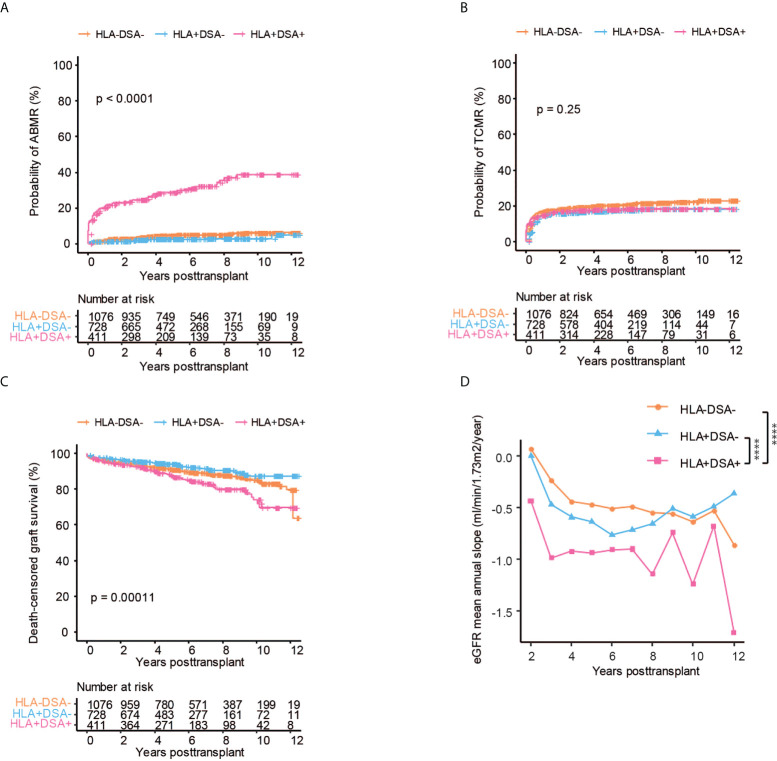
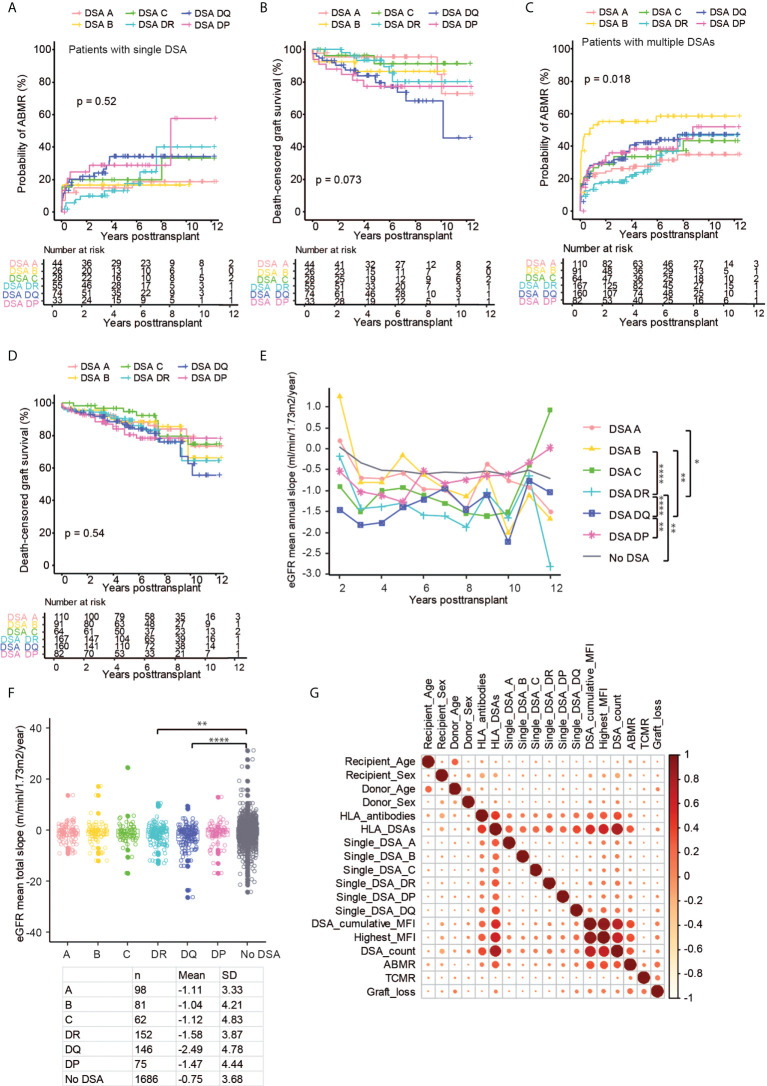
Methods: We investigated the effect of pre-transplant DSA on the risk of antibody-mediated rejection (ABMR), graft loss, and the rate of eGFR decline in 411 DSA positive transplants and 1804 DSA negative controls.
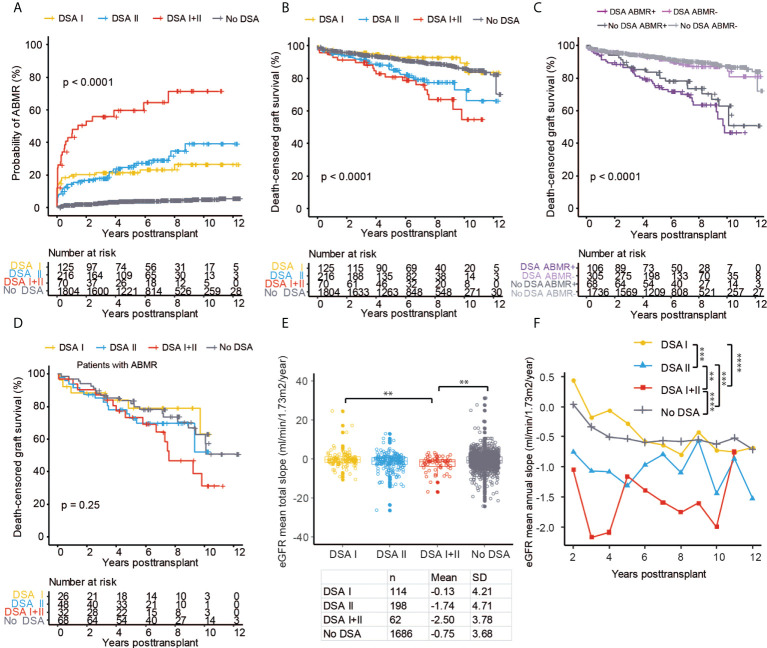
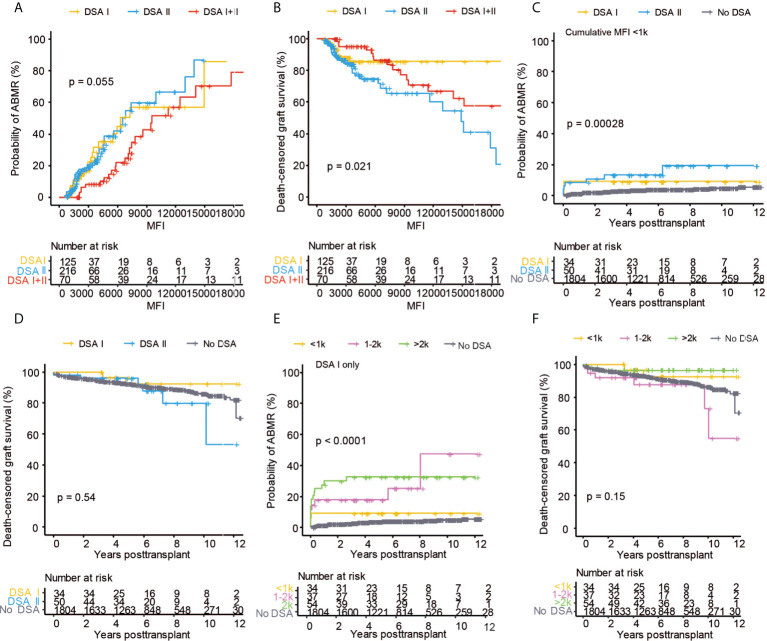
Results: Pre-transplant DSA were associated with a significantly increased risk of ABMR, graft loss, and accelerated eGFR decline. DSA directed at Class I and Class II HLA antigens were strongly associated with increased risk of ABMR, but only DSA directed at Class II associated with graft loss. DSA MFI markedly affected outcome, and Class II DSA were associated with ABMR already at 500-1000 MFI, whereas Class I DSA did not affect outcome at similar low MFI values. Furthermore, isolated DSA against HLA-DP carried comparable risks for ABMR, accelerated eGFR decline, and graft loss as DSA against HLA-DR.
Conclusion: Our results have important implications for the construction and optimization of vXM algorithms used within organ allocation systems. Our data suggest that both the HLA antigen target of the detected DSA as well as the cumulative MFI should be considered and that different MFI cut-offs could be considered for Class I and Class II directed DSA.
Keywords: abmr; donor specific antibodies; graft loss; kidney transplantation; virtual cross-match.
Copyright © 2022 Frischknecht, Deng, Wehmeier, de Rougemont, Villard, Ferrari-Lacraz, Golshayan, Gannagé, Binet, Wirthmueller, Sidler, Schachtner, Schaub, Nilsson and the Swiss Transplant Cohort Study.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous