

Sum of boxes of the clinical dementia rating scale highly predicts conversion or reversion in predementia stages
- PMID: 36212036
- PMCID: PMC9537043
- DOI: 10.3389/fnagi.2022.1021792
Sum of boxes of the clinical dementia rating scale highly predicts conversion or reversion in predementia stages
Abstract
Background: The clinical dementia rating (CDR) scale is commonly used to diagnose dementia due to Alzheimer's disease (AD). The sum of boxes of the CDR (CDR-SB) has recently been emphasized and applied to interventional trials for tracing the progression of cognitive impairment (CI) in the early stages of AD. We aimed to study the influence of baseline CDR-SB on disease progression to dementia or reversion to normal cognition (NC).
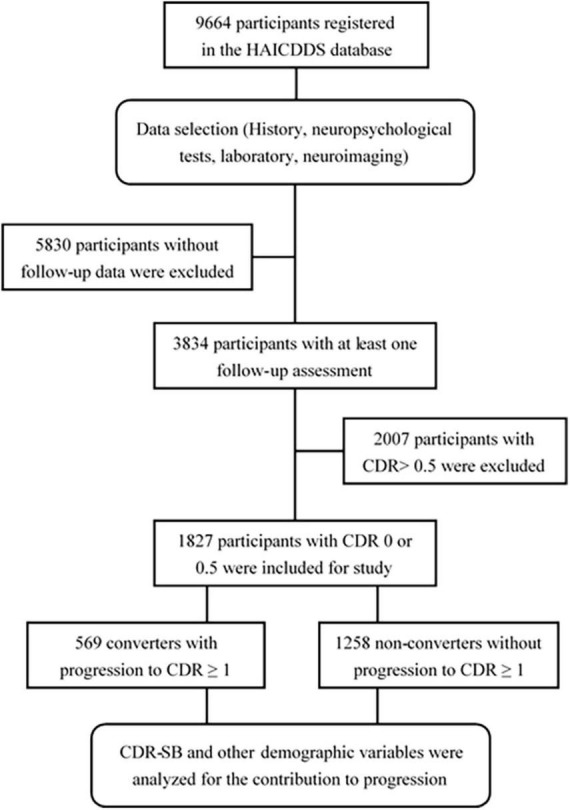
Materials and methods: The baseline CDR < 1 cohort registered from September 2015 to August 2020 with longitudinal follow-up in the History-based Artificial Intelligence Clinical Dementia Diagnostic System (HAICDDS) database was retrospectively analyzed for the rates of conversion to CDR ≥ 1. A Cox regression model was applied to study the influence of CDR-SB levels on progression, adjusting for age, education, sex, neuropsychological tests, neuropsychiatric symptoms, parkinsonism, and multiple vascular risk factors.
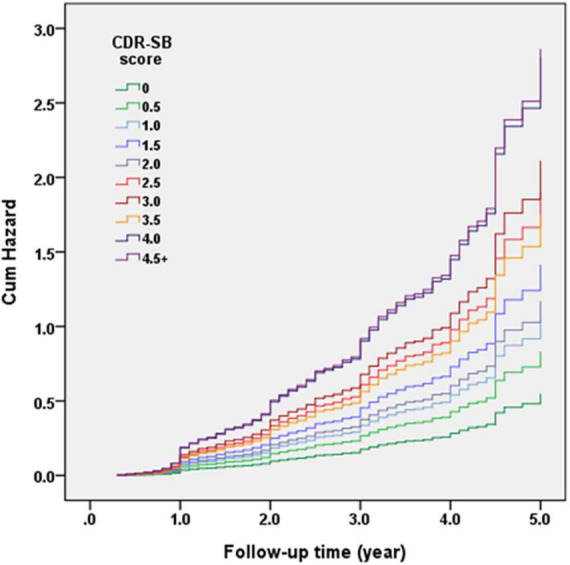
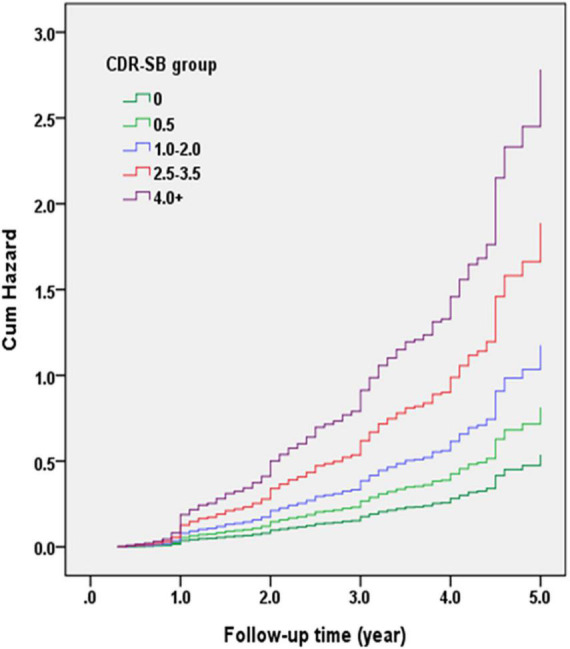
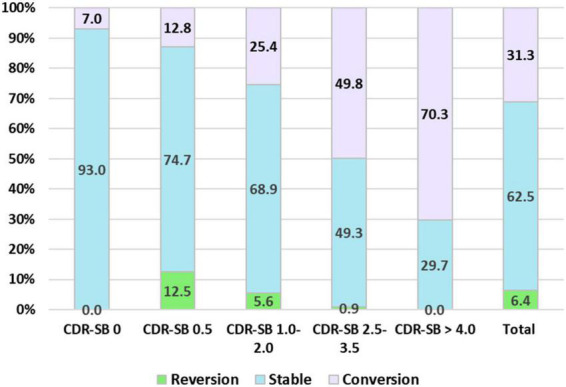
Results: A total of 1,827 participants were analyzed, including 1,258 (68.9%) non-converters, and 569 (31.1%) converters with mean follow-up of 2.1 (range 0.4-5.5) and 1.8 (range 0.3-5.0) years, respectively. Conversion rates increased with increasing CDR-SB scores. Compared to a CDR-SB score of 0, the hazard ratios (HR) for conversion to dementia were 1.51, 1.91, 2.58, 2.13, 3.46, 3.85, 3.19, 5.12, and 5.22 for CDR-SB scores of 0.5, 1.0, 1.5, 2.0, 2.5, 3.0, 3.5, 4.0, and ≥4.5, respectively (all p < 0.05 except for CDR-SB score = 0.5). In addition, older age, lower education, lower cognitive performance, and a history of diabetes also increased conversion rates. Furthermore, reversions to NC were 12.5, 5.6, 0.9, and 0% for CDR-SB scores of 0.5, 1.0-2.0, 2.5-3.5 and ≥4.0, respectively (p < 0.001).
Conclusion: CDR-SB in predementia or very mild dementia (VMD) stages highly predicts progression to dementia or reversion to NC. Therefore, CDR-SB could be a good candidate for tracing the effectiveness of pharmacological and non-pharmacological interventions in populations without dementia.
Keywords: Alzheimer’s disease; history-based artificial intelligence clinical dementia diagnostic system; predementia; sum of boxes of the clinical dementia rating; the clinical dementia rating.
Copyright © 2022 Tzeng, Yang, Hsu, Chang and Chiu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Operational Determination of Subjective Cognitive Decline, Mild Cognitive Impairment, and Dementia Using Sum of Boxes of the Clinical Dementia Rating Scale.Front Aging Neurosci. 2021 Sep 7;13:705782. doi: 10.3389/fnagi.2021.705782. eCollection 2021. Front Aging Neurosci. 2021. PMID: 34557083 Free PMC article.
-
Informant characteristics are associated with the Clinical Dementia Rating Sum of Boxes scores in the Alzheimer's Disease patients participating in the National Alzheimer's Coordinating Center Uniform Data Set.Res Sq [Preprint]. 2024 Mar 15:rs.3.rs-3982448. doi: 10.21203/rs.3.rs-3982448/v1. Res Sq. 2024. Update in: Nat Aging. 2024 Nov;4(11):1538-1543. doi: 10.1038/s43587-024-00732-x. PMID: 38559129 Free PMC article. Updated. Preprint.
-
Predicting the time to clinically worsening in mild cognitive impairment patients and its utility in clinical trial design by modeling a longitudinal clinical dementia rating sum of boxes from the ADNI database.J Alzheimers Dis. 2014;40(4):967-79. doi: 10.3233/JAD-132090. J Alzheimers Dis. 2014. PMID: 24531162
-
Stages of Objective Memory Impairment Predict Alzheimer's Disease Neuropathology: Comparison with the Clinical Dementia Rating Scale-Sum of Boxes.J Alzheimers Dis. 2021;80(1):185-195. doi: 10.3233/JAD-200946. J Alzheimers Dis. 2021. PMID: 33492286 Free PMC article.
-
Minimal clinically important difference in Alzheimer's disease: Rapid review.Alzheimers Dement. 2024 May;20(5):3352-3363. doi: 10.1002/alz.13770. Epub 2024 Apr 1. Alzheimers Dement. 2024. PMID: 38561021 Free PMC article.
Cited by
-
The Value of Subjective Olfactometry as a Predictive Biomarker of Neurodegenerative Diseases: A Systematic Review.Life (Basel). 2024 Feb 23;14(3):298. doi: 10.3390/life14030298. Life (Basel). 2024. PMID: 38541625 Free PMC article. Review.
-
Walking reduces the risk of dementia in patients with Parkinson's disease: a longitudinal follow-up study.Ther Adv Neurol Disord. 2025 Apr 12;18:17562864251330251. doi: 10.1177/17562864251330251. eCollection 2025. Ther Adv Neurol Disord. 2025. PMID: 40291756 Free PMC article.
-
Higher p-Cresol sulfate and tumor necrosis factor (TNF)-α levels are associated with cognitive improvement through increased TNF receptor 2 in individuals with mild cognitive impairment: A cross-sectional mediation analysis.J Alzheimers Dis Rep. 2025 Jul 24;9:25424823251362483. doi: 10.1177/25424823251362483. eCollection 2025 Jan-Dec. J Alzheimers Dis Rep. 2025. PMID: 40727257 Free PMC article.
-
Non-linear relationship between serum cholesterol levels and cognitive change among older people in the preclinical and prodromal stages of dementia: a retrospective longitudinal study in Taiwan.BMC Geriatr. 2024 May 30;24(1):474. doi: 10.1186/s12877-024-05030-0. BMC Geriatr. 2024. PMID: 38816835 Free PMC article.
-
Cerebral white matter lesions and regional blood flow are associated with reduced cognitive function in early-stage cognitive impairment.Front Aging Neurosci. 2023 Feb 16;15:1126618. doi: 10.3389/fnagi.2023.1126618. eCollection 2023. Front Aging Neurosci. 2023. PMID: 36875693 Free PMC article.
References
-
- Albert M. S., DeKosky S. T., Dickson D., Dubois B., Feldman H. H., Fox N. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7 270–279. 10.1016/j.jalz.2011.03.008 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical