

Risk factors and predictive nomograms for early death of patients with pancreatic cancer liver metastasis: A large cohort study based on the SEER database and Chinese population
- PMID: 36212438
- PMCID: PMC9539004
- DOI: 10.3389/fonc.2022.998445
Risk factors and predictive nomograms for early death of patients with pancreatic cancer liver metastasis: A large cohort study based on the SEER database and Chinese population
Abstract
Background: The liver is the most common organ for distant metastasis of pancreatic cancer, and patients with pancreatic cancer liver metastases (PCLM) often die in a short period of time. As such, the establishment of an effective nomogram to predict the probability of early death (survival time ≤3 months) in PCLM patients is of considerable significance.
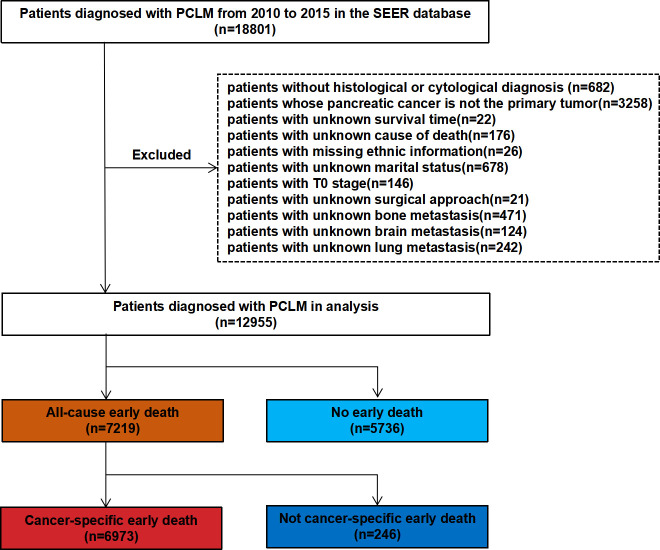
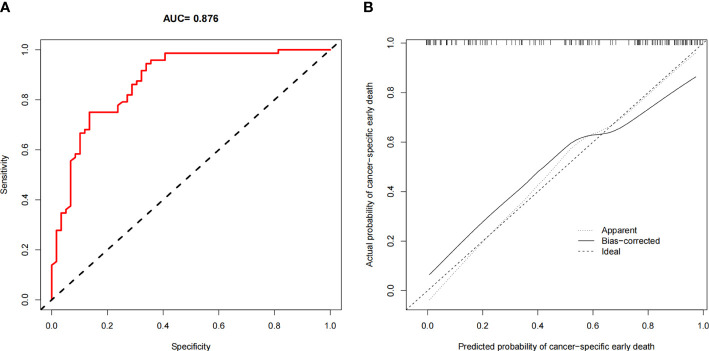
Methods: Patients diagnosed with PCLM in the Surveillance, Epidemiology, and End Result (SEER) database between 2010 and 2015 were included for model construction and internal validation. A data set was obtained from the Chinese population for external validation. Risk factors that contributed to all-cause and cancer-specific early death were determined by means of univariable and multivariable logistic regression. The accuracy of the nomogram was verified by means of receiver operating characteristic (ROC) curves, and the true consistency of the model was assessed by calibration curves. The clinical applicability of the model was evaluated by means of decision curve analysis (DCA).
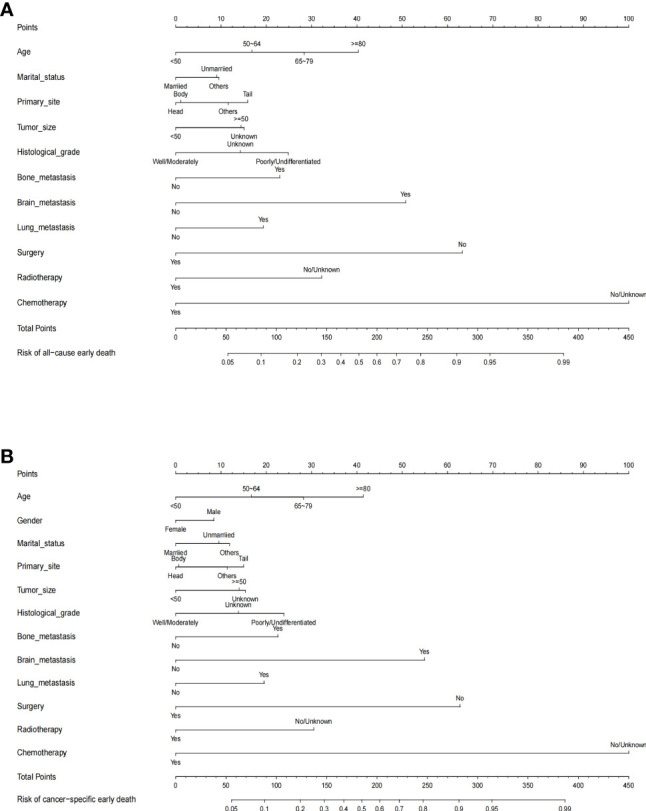
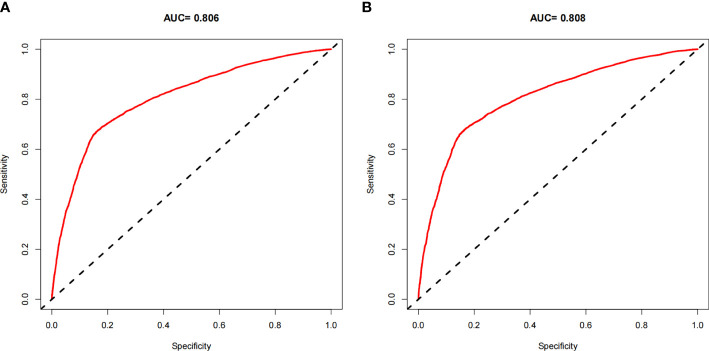
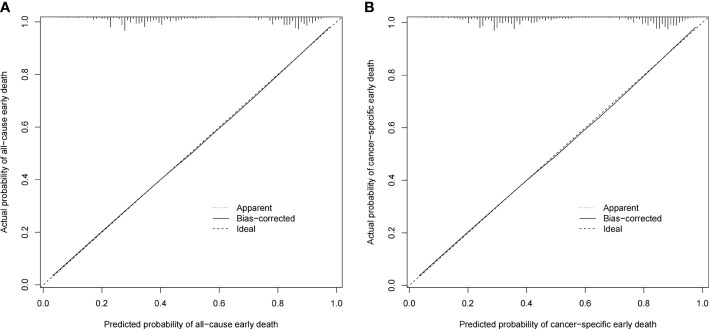
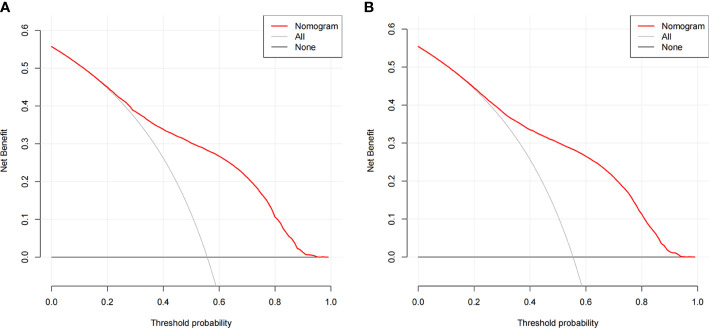
Results: A total of 12,955 patients were included in the present study, of whom 7,219 (55.7%) experienced early death and 6,973 (53.8%) patients died of PCLM. Through multivariable logistic regression analysis, 11 risk factors associated with all-cause early death and 12 risk factors associated with cancer-specific early death were identified. The area under the curves (AUCs) for all-cause and cancer-specific early death were 0.806 (95% CI: 0.785- 0.827) and 0.808 (95% CI: 0.787- 0.829), respectively. Internal validation showed that the C-indexes of all-cause and cancer-specific early death after bootstrapping (5,000 re-samplings) were 0.805 (95% CI: 0.784-0.826) and 0.807 (95% CI: 0.786-0.828), respectively. As revealed by the calibration curves, the constructed nomograms exhibited good consistency. The decision curve analysis (DCA) indicated the nomograms had significant clinical applicability.
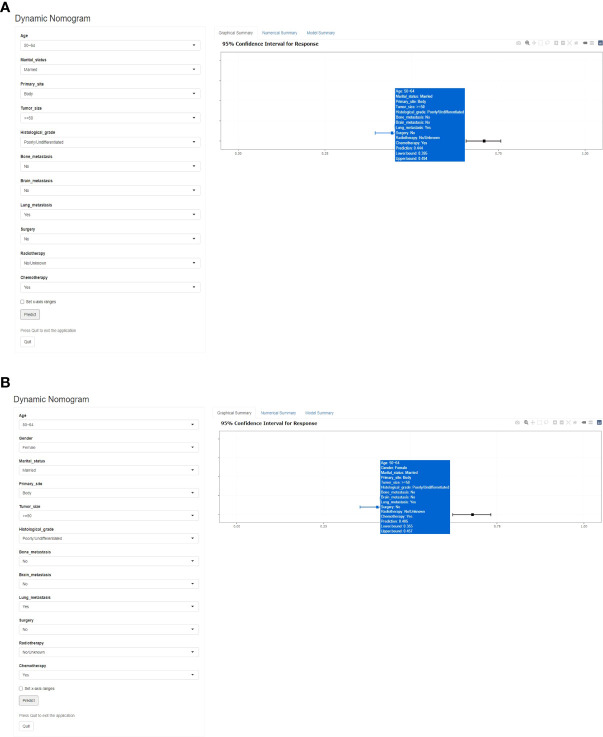
Conclusion: In the present study, reliable nomograms were developed for predicting the early death probability in patients with PCLM. Such tools can help clinicians identify high-risk patients and develop individualized treatment plans as early as possible.
Keywords: SEER database; early death; liver metastasis; nomogram; pancreatic cancer.
Copyright © 2022 Zhang, Dong, Pan, Du, Liu, Xu and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Two Novel Nomograms Predicting the Risk and Prognosis of Pancreatic Cancer Patients With Lung Metastases: A Population-Based Study.Front Public Health. 2022 May 31;10:884349. doi: 10.3389/fpubh.2022.884349. eCollection 2022. Front Public Health. 2022. PMID: 35712294 Free PMC article.
-
Nomograms for Predicting the Risk and Prognosis of Liver Metastases in Pancreatic Cancer: A Population-Based Analysis.J Pers Med. 2023 Feb 24;13(3):409. doi: 10.3390/jpm13030409. J Pers Med. 2023. PMID: 36983591 Free PMC article.
-
Risk factors, prognostic predictors, and nomograms for pancreatic cancer patients with initially diagnosed synchronous liver metastasis.World J Gastrointest Oncol. 2023 Jan 15;15(1):128-142. doi: 10.4251/wjgo.v15.i1.128. World J Gastrointest Oncol. 2023. PMID: 36684042 Free PMC article.
-
Risk factors and predictive nomograms for early death of patients with advanced hepatocellular carcinoma: a large retrospective study based on the SEER database.BMC Gastroenterol. 2022 Jul 19;22(1):348. doi: 10.1186/s12876-022-02424-5. BMC Gastroenterol. 2022. PMID: 35854221 Free PMC article.
-
Risk factors and survival prediction of pancreatic cancer with lung metastases: A population-based study.Front Oncol. 2022 Sep 21;12:952531. doi: 10.3389/fonc.2022.952531. eCollection 2022. Front Oncol. 2022. PMID: 36212473 Free PMC article.
Cited by
-
Development and validation of a prognostic nomogram for ovarian clear cell carcinoma: a study based on the SEER database and a Chinese cohort.Discov Oncol. 2025 Apr 7;16(1):482. doi: 10.1007/s12672-025-02272-1. Discov Oncol. 2025. PMID: 40192950 Free PMC article.
-
Machine learning was used to predict risk factors for distant metastasis of pancreatic cancer and prognosis analysis.J Cancer Res Clin Oncol. 2023 Sep;149(12):10279-10291. doi: 10.1007/s00432-023-04903-y. Epub 2023 Jun 6. J Cancer Res Clin Oncol. 2023. PMID: 37278826 Free PMC article.
-
Development and validation of machine learning nomograms for predicting survival in stage IV pancreatic cancer: A retrospective study.World J Gastrointest Oncol. 2025 May 15;17(5):102459. doi: 10.4251/wjgo.v17.i5.102459. World J Gastrointest Oncol. 2025. PMID: 40487945 Free PMC article.
-
A novel nomogram and risk classification system based on inflammatory and immune indicators for predicting prognosis of pancreatic cancer patients with liver metastases.Cancer Med. 2023 Sep;12(18):18622-18632. doi: 10.1002/cam4.6471. Epub 2023 Aug 27. Cancer Med. 2023. PMID: 37635391 Free PMC article.
References
-
- Oweira H, Petrausch U, Helbling D, Schmidt J, Mannhart M, Mehrabi A, et al. . Prognostic value of site-specific metastases in pancreatic adenocarcinoma: A surveillance epidemiology and end results database analysis. World J Gastroenterol (2017) 23(10):1872–80. doi: 10.3748/wjg.v23.i10.1872 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials