

Can circulating PD-1, PD-L1, BTN3A1, pan-BTN3As, BTN2A1 and BTLA levels enhance prognostic power of CA125 in patients with advanced high-grade serous ovarian cancer?
- PMID: 36212445
- PMCID: PMC9532861
- DOI: 10.3389/fonc.2022.946319
Can circulating PD-1, PD-L1, BTN3A1, pan-BTN3As, BTN2A1 and BTLA levels enhance prognostic power of CA125 in patients with advanced high-grade serous ovarian cancer?
Abstract
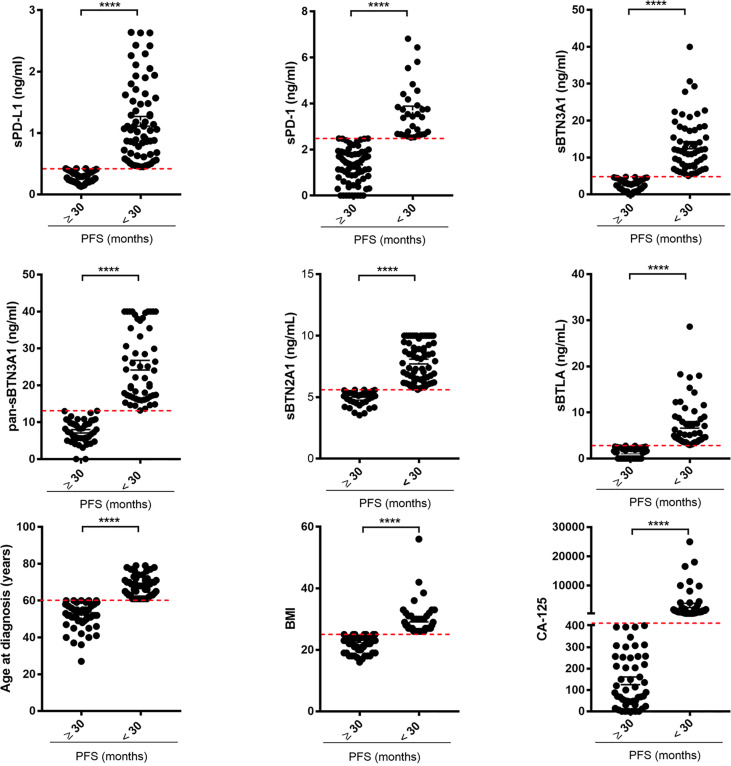
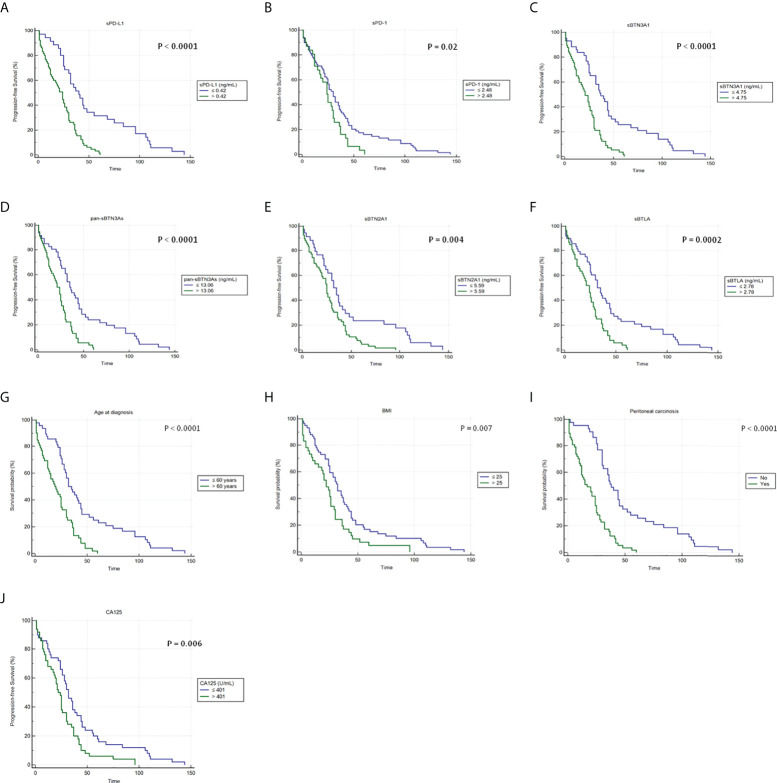
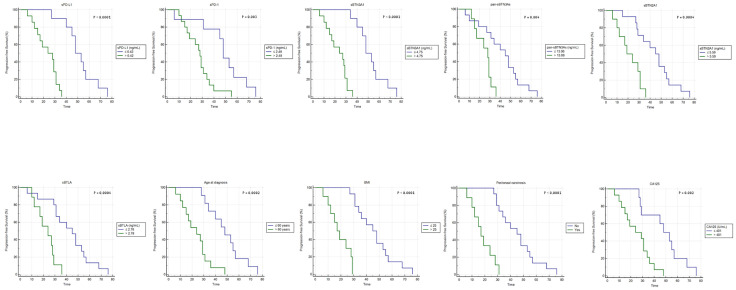
The most common subtype of ovarian cancer (OC) is the high-grade serous ovarian carcinoma (HGSOC), accounting for 70%-80% of all OC deaths. Although HGSOC is a potentially immunogenic tumor, clinical studies assessing the effectiveness of inhibitors of programmed death protein and its ligand (PD-1/PD-L1) in OC patients so far showed only response rates <15%. However, recent studies revealed an interesting prognostic role of plasma PD-1/PD-L1 and other circulating immunoregulatory molecules, such as the B- and T-lymphocyte attenuator (BTLA), butyrophilin sub-family 3A/CD277 receptors (BTN3A), and butyrophilin sub-family 2 member A1 (BTN2A1), in several solid tumors. Since evidence showed the prognostic relevance of pretreatment serum CA125 levels in OC, the aim of our study was to investigate if soluble forms of inhibitory immune checkpoints can enhance prognostic power of CA125 in advanced HGSOC women. Using specific ELISA tests, we examined the circulating PD-1, PD-L1, pan-BTN3As, BTN3A1, BTN2A1, and BTLA levels in 100 advanced HGSOC patients before treatment, correlating them with baseline serum CA125, age at diagnosis, body mass index (BMI), and peritoneal carcinomatosis. A multivariate analysis revealed that plasma BTN3A1 ≤4.75 ng/ml (HR, 1.94; 95% CI, 1.23-3.07; p=0.004), age at diagnosis ≤60 years (HR, 1.65; 95% CI, 1.05-2.59; p=0.03) and absence of peritoneal carcinomatosis (HR, 2.65; 95% CI, 1.66-4.22; p<0.0001) were independent prognostic factors for a longer progression-free survival (PFS) (≥30 months) in advanced HGSOC women. However, further two-factor multivariate analyses highlighted that baseline serum CA125 levels >401 U/ml and each soluble protein above respective concentration cutoff were covariates associated with shorter PFS (<30 months) and unfavorable clinical outcome, suggesting that contemporary measurement of both biomarkers than CA125 only could strengthen prognostic power of serum CA125 in predicting PFS of advanced HGSOC women. Plasma PD-L1, PD-1, BTN3A1, pan-sBTN3As, BTN2A1, or BTLA levels could be helpful biomarkers to increase prognostic value of CA125.
Keywords: BTLA; HGSOC; PD-1; PD-L1; butyrophilins; circulating immune checkpoints; prognostic factors; serum CA125.
Copyright © 2022 Fanale, Corsini, Brando, Cutaia, Di Donna, Filorizzo, Lisanti, Randazzo, Magrin, Romano, Bazan Russo, Olive, Vieni, Pantuso, Chiantera, Russo, Bazan and Iovanna.
Conflict of interest statement
JLI is cofounder of PanCa Therapeutics and PredicitngMed. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous