

Psychiatrization in mental health care: The emergency department
- PMID: 36213516
- PMCID: PMC9538185
- DOI: 10.3389/fsoc.2022.793836
Psychiatrization in mental health care: The emergency department
Abstract
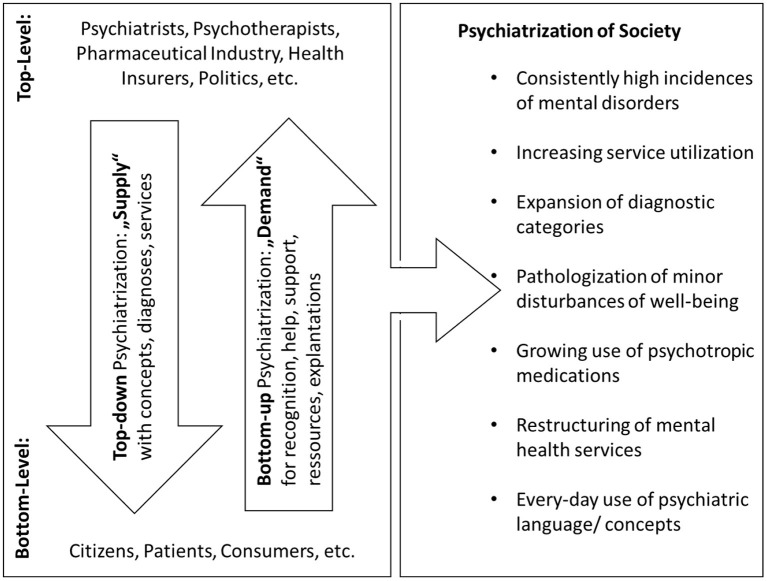
Background: In the light of high incidences of diagnosed mental disorders and the growing utilization of mental healthcare services, a progressing psychiatrization of society has been hypothesized as the underlying dynamic of these developments. Mental healthcare institutions, such as psychiatric hospitals, may play a decisive role in this. However, there is a scarcity of research into how psychiatrization emerges in hospital settings. This paper explores whether the emergency department (ED) can be considered as a site where psychiatrization happens, becomes observable, and which factors in the context of the ED may be its potential drivers.
Methods: Two cases as encountered in an interdisciplinary ED will be presented in the following in an anonymized way. Although the cases originate from individual consultations, they can be considered as prototypical. The cases were collected and discussed using the method of interactive interviewing. The results will be analyzed against the backdrop of current theoretic concepts of psychiatrization.
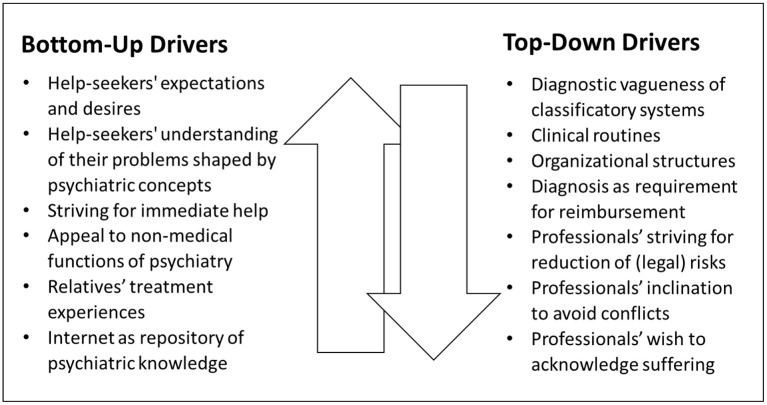
Findings: The ED can be seen as an important area of contact between society and psychiatry. Decisions whether to label a certain condition as a "mental disorder" and to therefore initiate psychiatric treatment, or not, can be highly difficult, especially in cases where the (health) concerns are rather moderate, and clearly associated with common life problems. Psychiatrists' decisions may be largely influenced in favor of psychiatrization by a wide array of disciplinary, institutional, interpersonal, personal, cultural, and social factors.
Conclusions: The ED appears to be a promising field for research into the mechanisms and motives through which psychiatrization may emerge in mental healthcare settings. Psychiatrists in the ED work within a complex sphere of top-down and bottom-up drivers of psychiatrization. Encounters in the ED can be an important step toward adequate support for many individuals, but they also risk becoming the starting point of psychiatrization by interpreting certain problems through the psychiatric gaze, which may induce diagnoses of questionable validity and treatment of little use.
Keywords: case study; emergency care; health system research; medicalization; overdiagnosis; psychiatric epidemiology; psychiatrization; transdisciplinary research.
Copyright © 2022 Beeker.
Conflict of interest statement
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Abraham J. (2010). Pharmaceuticalization of society in context: theoretical, empirical and health dimensions. Sociology 44, 603–622. 10.1177/0038038510369368 - DOI
-
- Adams T. E. (2008). A review of narrative ethics. Qual. Inq. 14, 175–194. 10.1177/1077800407304417 - DOI
-
- Améry J. (1976). On Suicide: A Discourse on Voluntary Death. Bloomington: Indiana University Press.
-
- Ariès P. (1974). Western Attitudes Toward Death From the Middle Ages to the Present. Baltimore: Johns Hopkins University Press.
LinkOut - more resources
Full Text Sources