

Preliminary study: quantification of chronic pain from physiological data
- PMID: 36213596
- PMCID: PMC9534370
- DOI: 10.1097/PR9.0000000000001039
Preliminary study: quantification of chronic pain from physiological data
Abstract
Introduction: It is unknown if physiological changes associated with chronic pain could be measured with inexpensive physiological sensors. Recently, acute pain and laboratory-induced pain have been quantified with physiological sensors.
Objectives: To investigate the extent to which chronic pain can be quantified with physiological sensors.
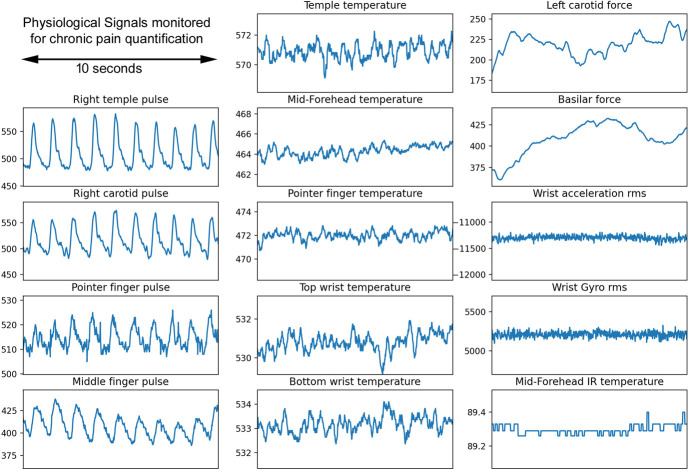
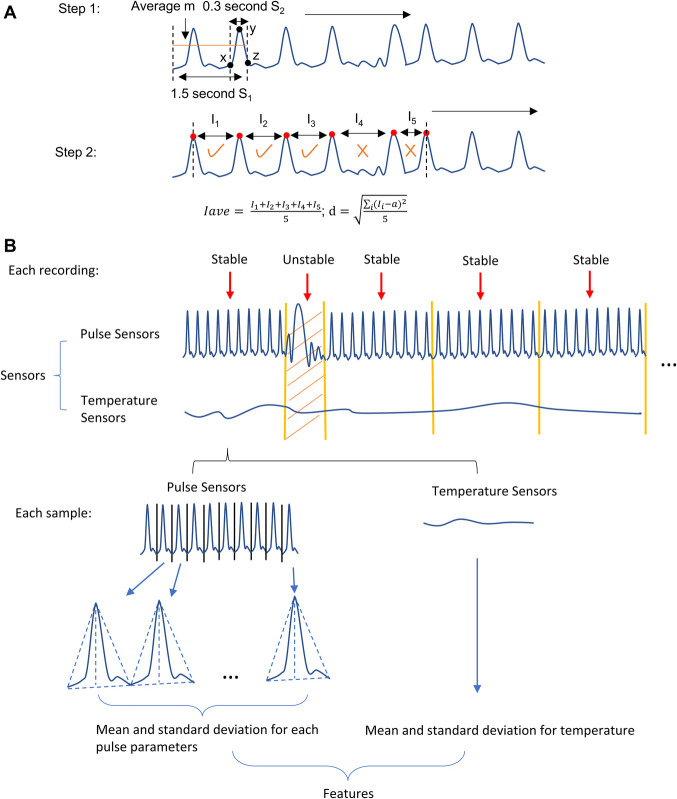
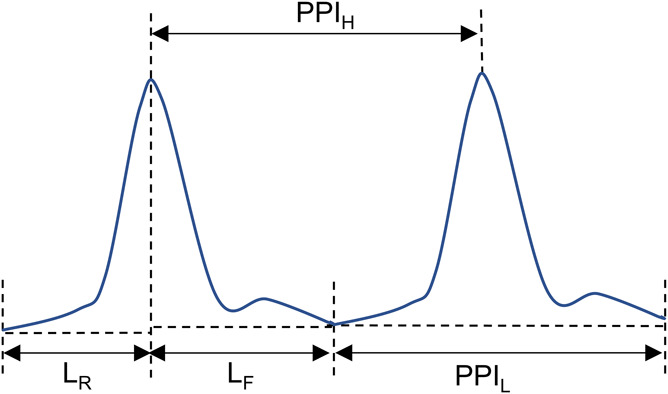
Methods: Data were collected from chronic pain sufferers who subjectively rated their pain on a 0 to 10 visual analogue scale, using our recently developed pain meter. Physiological variables, including pulse, temperature, and motion signals, were measured at head, neck, wrist, and finger with multiple sensors. To quantify pain, features were first extracted from 10-second windows. Linear models with recursive feature elimination were fit for each subject. A random forest regression model was used for pain score prediction for the population-level model.
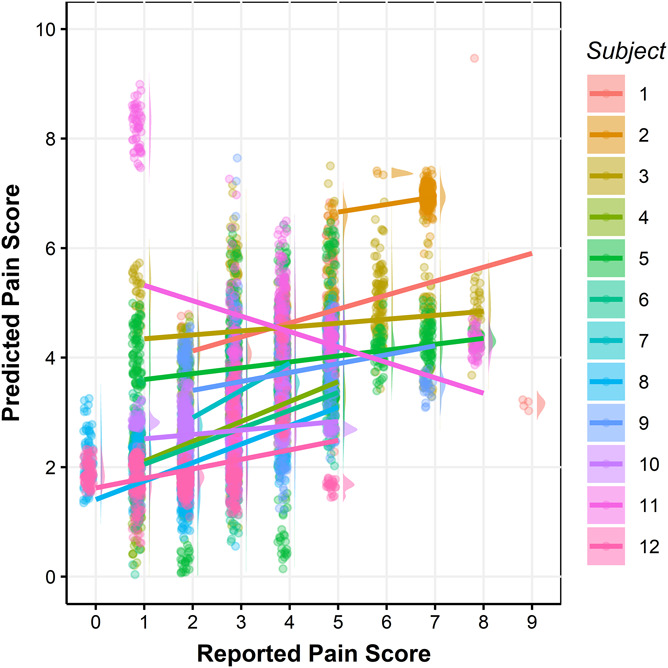
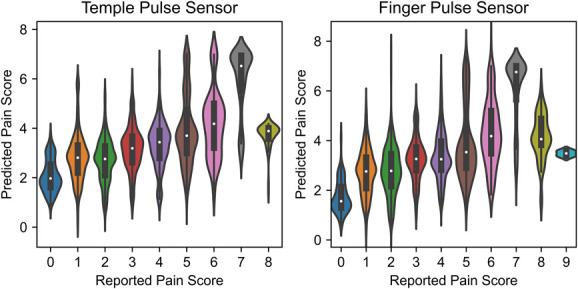
Results: Predictive performance was assessed using leave-one-recording-out cross-validation and nonparametric permutation testing. For individual-level models, 5 of 12 subjects yielded intraclass correlation coefficients between actual and predicted pain scores of 0.46 to 0.75. For the population-level model, the random forest method yielded an intraclass correlation coefficient of 0.58. Bland-Altman analysis shows that our model tends to overestimate the lower end of the pain scores and underestimate the higher end.
Conclusion: This is the first demonstration that physiological data can be correlated with chronic pain, both for individuals and populations. Further research and more extensive data will be required to assess whether this approach could be used as a "chronic pain meter" to assess the level of chronic pain in patients.
Keywords: Chronic pain; Pain quantification; Physiological data; Random forest.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The International Association for the Study of Pain.
Conflict of interest statement
The authors have no conflicts of interest to declare.Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures

References
-
- Åkerblom S, Perrin S, Fischer MR, McCracken LM. Treatment outcomes in group-based cognitive behavioural therapy for chronic pain: an examination of PTSD symptoms. Eur J Pain 2020;24:807–17. - PubMed