

Changing Critical Care Patterns and Associated Outcomes in Mechanically Ventilated Severe COVID-19 Patients in Different Time Periods: An Explanatory Study from Central India
- PMID: 36213712
- PMCID: PMC9492749
- DOI: 10.5005/jp-journals-10071-24279
Changing Critical Care Patterns and Associated Outcomes in Mechanically Ventilated Severe COVID-19 Patients in Different Time Periods: An Explanatory Study from Central India
Abstract
Background: The outcomes in critical illness depend on disease severity, practice protocols, workload, and access to care. This study investigates the factors affecting outcomes in mechanically ventilated coronavirus disease-2019 acute respiratory distress syndrome (COVID-19 ARDS) patients admitted in a tertiary teaching hospital intensive care unit (ICU) in Central India with reference to different time periods in pandemic. This is one of the largest series of mechanically ventilated COVID-19 ARDS patients, globally.
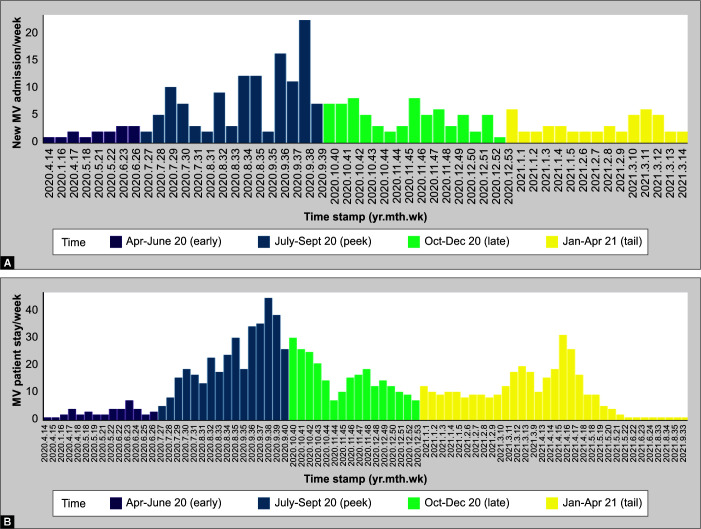
Methods: This retrospective cohort study classified the entire data into four time periods (Period 1: April 2020 to June 2020; Period 2: July 2020 to September 2020; Period 3: October 2020 to December 2020; and Period 4: January 2021 to April 2021). We performed a multivariable-adjusted analysis to evaluate predictors of mortality, adjusted for baseline-severity, sequential organ failure assessment (SOFA score) and time period. We applied mixed-effect binomial logistic regression to model fixed-effect variables with incremental complexity.
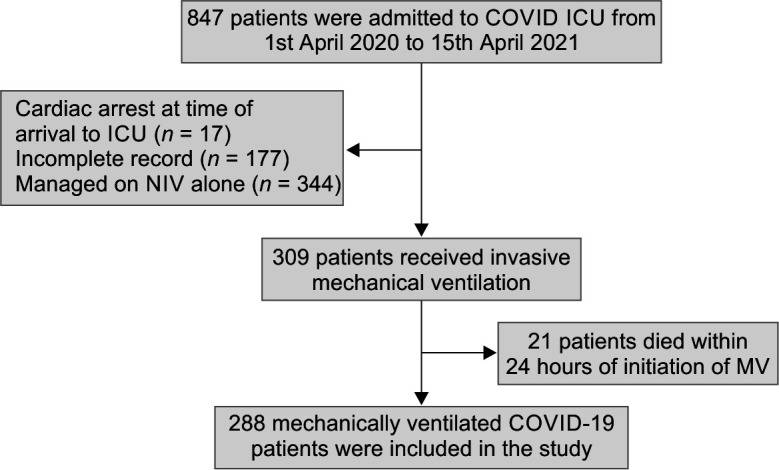
Results: Among the 56 survivors (19.4%) out of 288 mechanically ventilated patients, there was an up-gradient of survival proportion (0, 18.2, 17.4, and 28.6%) in four time periods. Symptom-intubation interval (OR 1.16; 95% CI 1.03-1.31) and driving pressures (DPs) (OR 1.17; 95% CI 1.07-1.28) were significant predictors of mortality in the model having minimal AIC and BIC values. Patients aged above 60 years also had a larger effect, but statistically insignificant effect favoring mortality (OR 1.99; 95% CI 0.92-4.27). The most complex but less parsimonious model (with higher AIC/BIC) indicated the protective odds of high steroid on mortality (OR 0.59; 95% CI 0.59-0.82).
Conclusion: The outcomes in mechanically ventilated COVID-19 ARDS patients are heterogeneous across time windows and may be affected by the complex interaction of baseline risk and critical care parameters.
How to cite this article: Saigal S, Joshi A, Panda R, Goyal A, Kodamanchili S, Anand A, et al. Changing Critical Care Patterns and Associated Outcomes in Mechanically Ventilated Severe COVID-19 Patients in Different Time Periods: An Explanatory Study from Central India. Indian J Crit Care Med 2022;26(9):1022-1030.
Keywords: Acute respiratory distress syndrome; Coronavirus disease-2019; Intensive care unit; Mechanical ventilation.
Copyright © 2022; The Author(s).
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures
Similar articles
-
Corticosteroid treatment and mortality in mechanically ventilated COVID-19-associated acute respiratory distress syndrome (ARDS) patients: a multicentre cohort study.Ann Intensive Care. 2021 Nov 26;11(1):159. doi: 10.1186/s13613-021-00951-0. Ann Intensive Care. 2021. PMID: 34825976 Free PMC article.
-
A Comparative Study on the Outcomes of Mechanically Ventilated COVID-19 vs Non-COVID-19 Patients with Acute Hypoxemic Respiratory Failure.Indian J Crit Care Med. 2021 Dec;25(12):1377-1381. doi: 10.5005/jp-journals-10071-24009. Indian J Crit Care Med. 2021. PMID: 35027797 Free PMC article.
-
Mechanical power and 30-day mortality in mechanically ventilated, critically ill patients with and without Coronavirus Disease-2019: a hospital registry study.J Intensive Care. 2023 Apr 6;11(1):14. doi: 10.1186/s40560-023-00662-7. J Intensive Care. 2023. PMID: 37024938 Free PMC article.
-
Protocol-directed sedation versus non-protocol-directed sedation in mechanically ventilated intensive care adults and children.Cochrane Database Syst Rev. 2018 Nov 12;11(11):CD009771. doi: 10.1002/14651858.CD009771.pub3. Cochrane Database Syst Rev. 2018. PMID: 30480753 Free PMC article.
-
Procedures in COVID-19 Patients: Part-I.Indian J Crit Care Med. 2020 Nov;24(Suppl 5):S263-S271. doi: 10.5005/jp-journals-10071-23597. Indian J Crit Care Med. 2020. PMID: 33354050 Free PMC article. Review.
Cited by
-
Changes in Driving Pressure vs Oxygenation as Predictor of Mortality in Moderate to Severe Acute Respiratory Distress Syndrome Patients Receiving Prone Position Ventilation.Indian J Crit Care Med. 2024 Feb;28(2):134-140. doi: 10.5005/jp-journals-10071-24643. Indian J Crit Care Med. 2024. PMID: 38323262 Free PMC article.
References
-
- Cook TM, El–Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia. 2020;75(6):785–799. doi: 10.1111/anae.15054. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous