

New and Progressive Medical Conditions After Pediatric Sepsis Hospitalization Requiring Critical Care
- PMID: 36215045
- PMCID: PMC9552050
- DOI: 10.1001/jamapediatrics.2022.3554
New and Progressive Medical Conditions After Pediatric Sepsis Hospitalization Requiring Critical Care
Abstract
Importance: Children commonly experience physical, cognitive, or emotional sequelae after sepsis. However, little is known about the development or progression of medical conditions after pediatric sepsis.
Objective: To quantify the development and progression of 4 common conditions in the 6 months after sepsis and to assess whether they differed after hospitalization for sepsis vs nonsepsis among critically ill children.
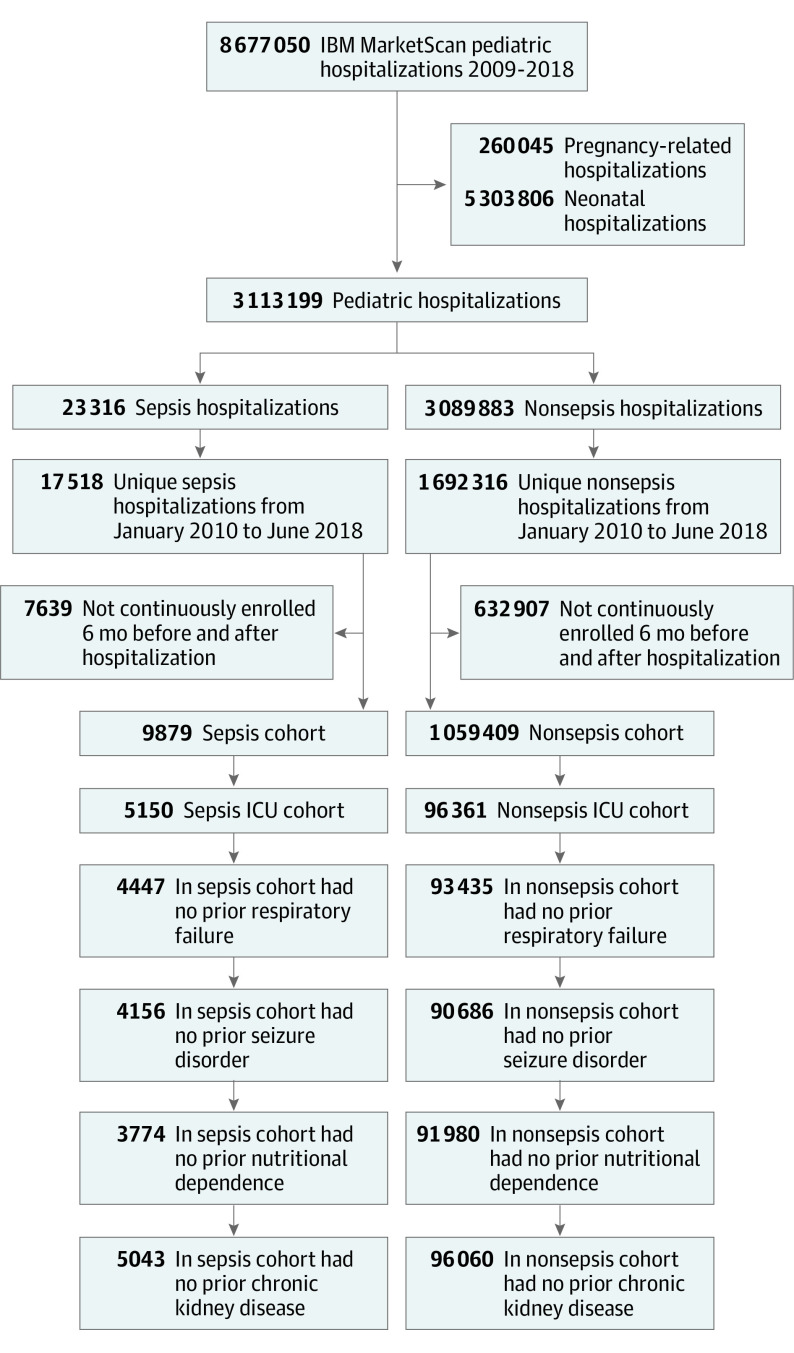
Design, setting, and participants: This cohort study of 101 511 children (<19 years) with sepsis or nonsepsis hospitalization used a national administrative claims database (January 1, 2010, to June 30, 2018). Data management and analysis were conducted from April 1, 2020, to July 7, 2022.
Exposures: Intensive care unit hospitalization for sepsis vs all-cause intensive care unit hospitalizations, excluding sepsis.
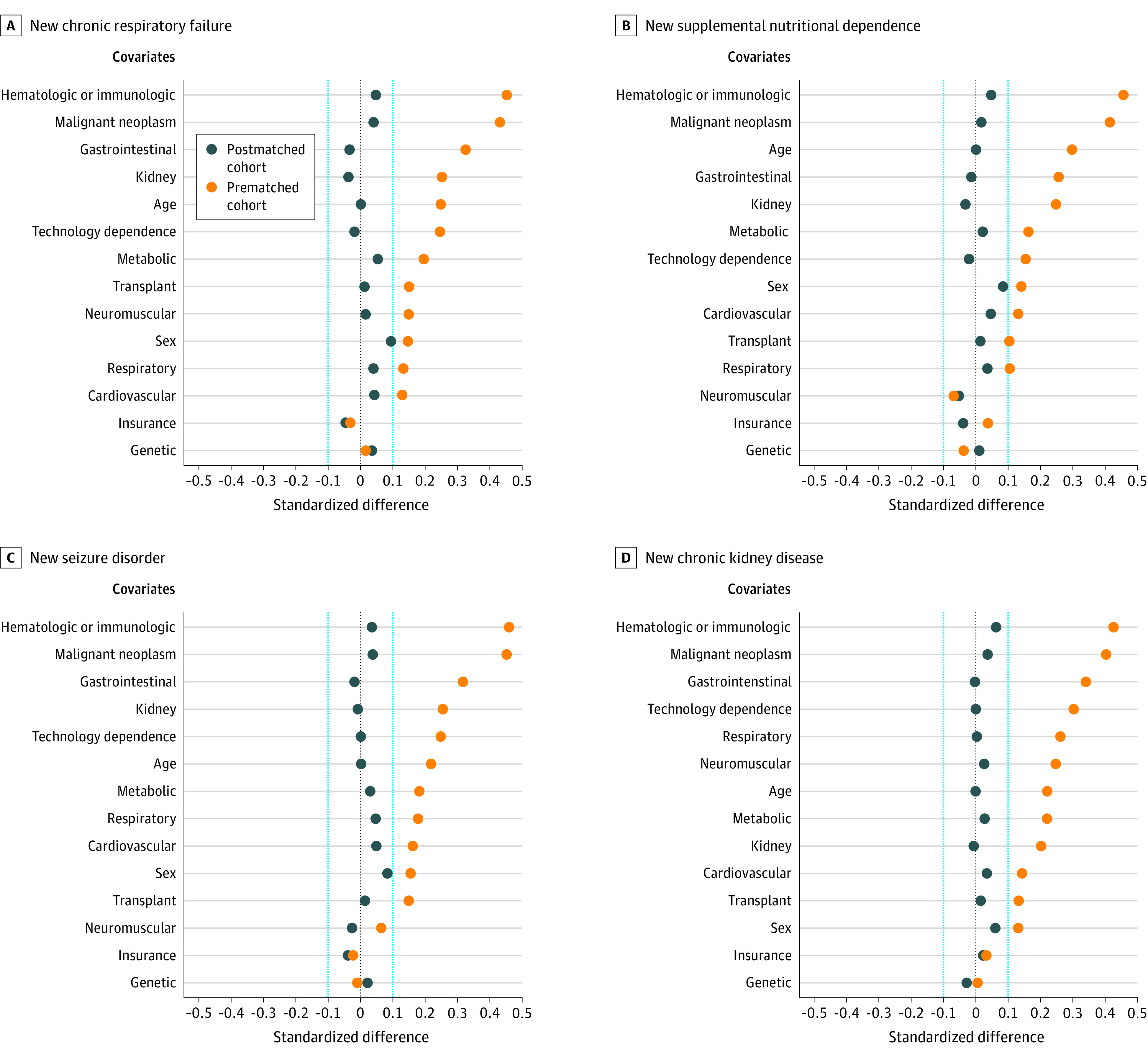
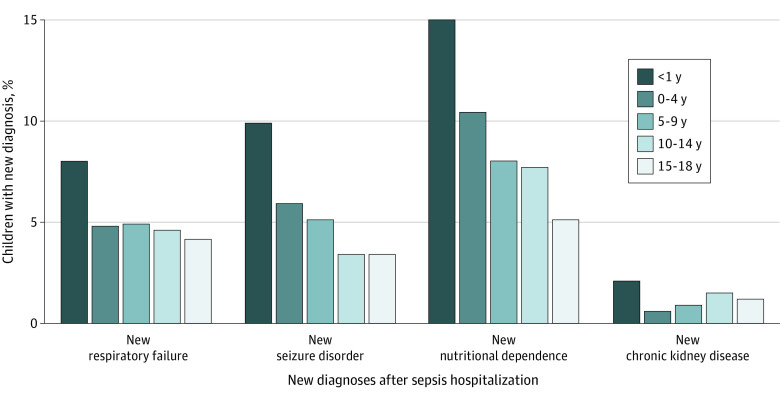
Main outcomes and measures: Primary outcomes were the development of 4 target conditions (chronic respiratory failure, seizure disorder, supplemental nutritional dependence, and chronic kidney disease) within 6 months of hospital discharge. Secondary outcomes were the progression of the 4 target conditions among children with the condition before hospitalization. Outcomes were identified via diagnostic and procedural codes, durable medical equipment codes, and prescription medications. Differences in the development and the progression of conditions between pediatric patients with sepsis and pediatric patients with nonsepsis who survived intensive care unit hospitalization were assessed using logistic regression with matching weights.
Results: A total of 5150 survivors of pediatric sepsis and 96 361 survivors of nonsepsis intensive care unit hospitalizations were identified; 2593 (50.3%) were female. The median age was 9.5 years (IQR, 3-15 years) in the sepsis cohort and 7 years (IQR, 2-13 years) in the nonsepsis cohort. Of the 5150 sepsis survivors, 670 (13.0%) developed a new target condition, and 385 of 1834 (21.0%) with a preexisting target condition had disease progression. A total of 998 of the 5150 survivors (19.4%) had development and/or progression of at least 1 condition. New conditions were more common among sepsis vs nonsepsis hospitalizations (new chronic respiratory failure: 4.6% vs 1.9%; odds ratio [OR], 2.54 [95% CI, 2.19-2.94]; new supplemental nutritional dependence: 7.9% vs 2.7%; OR, 3.17 [95% CI, 2.80-3.59]; and new chronic kidney disease: 1.1% vs 0.6%; OR, 1.65 [95% CI, 1.25-2.19]). New seizure disorder was less common (4.6% vs 6.0%; OR, 0.77 [95% CI, 0.66-0.89]). Progressive supplemental nutritional dependence was more common (1.5% vs 0.5%; OR, 2.95 [95% CI, 1.60-5.42]), progressive epilepsy was less common (33.7% vs 40.6%; OR, 0.74 [95% CI, 0.65-0.86]), and progressive respiratory failure (4.4% vs 3.3%; OR, 1.35 [95% CI, 0.89-2.04]) and progressive chronic kidney disease (7.9% vs 9.2%; OR, 0.84 [95% CI, 0.18-3.91]) were similar among survivors of sepsis vs nonsepsis admitted to an intensive care unit.
Conclusions and relevance: In this national cohort of critically ill children who survived sepsis, 1 in 5 developed or had progression of a condition of interest after sepsis hospitalization, suggesting survivors of pediatric sepsis may benefit from structured follow-up to identify and treat new or worsening medical comorbid conditions.
Conflict of interest statement
Figures
References
-
- Zimmerman JJ, Banks R, Berg RA, et al. ; Life After Pediatric Sepsis Evaluation (LAPSE) Investigators . Critical illness factors associated with long-term mortality and health-related quality of life morbidity following community-acquired pediatric septic shock. Crit Care Med. 2020;48(3):319-328. doi:10.1097/CCM.0000000000004122 - DOI - PMC - PubMed
-
- Zimmerman JJ, Banks R, Berg RA, et al. ; Life After Pediatric Sepsis Evaluation (LAPSE) Investigators . Trajectory of mortality and health-related quality of life morbidity following community-acquired pediatric septic shock. Crit Care Med. 2020;48(3):329-337. doi:10.1097/CCM.0000000000004123 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
