

Impact and Recovery from COVID-19-Related Disruptions in Colorectal Cancer Screening and Care in the US: A Scenario Analysis
- PMID: 36215205
- PMCID: PMC9827109
- DOI: 10.1158/1055-9965.EPI-22-0544
Impact and Recovery from COVID-19-Related Disruptions in Colorectal Cancer Screening and Care in the US: A Scenario Analysis
Abstract
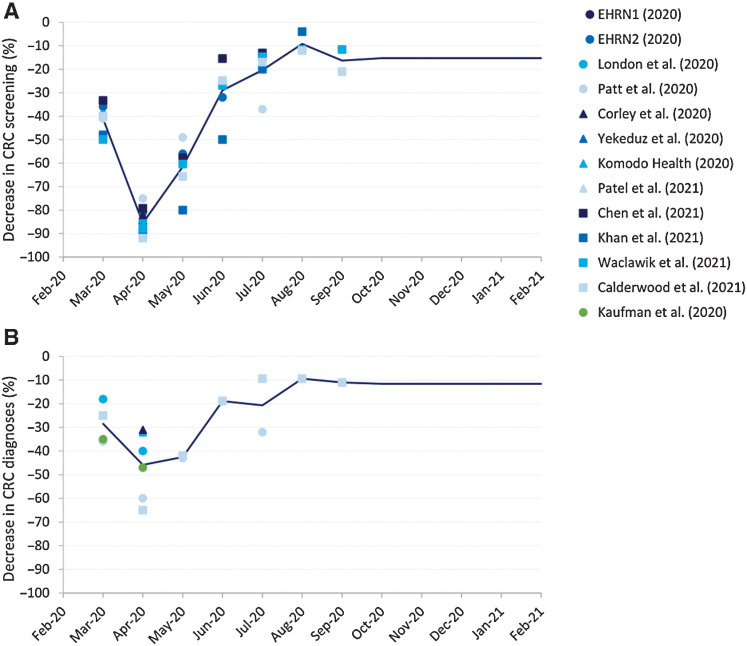
Background: Many colorectal cancer-related procedures were suspended during the COVID-19 pandemic. In this study, we predict the impact of resulting delays in screening (colonoscopy, FIT, and sigmoidoscopy) and diagnosis on colorectal cancer-related outcomes, and compare different recovery scenarios.
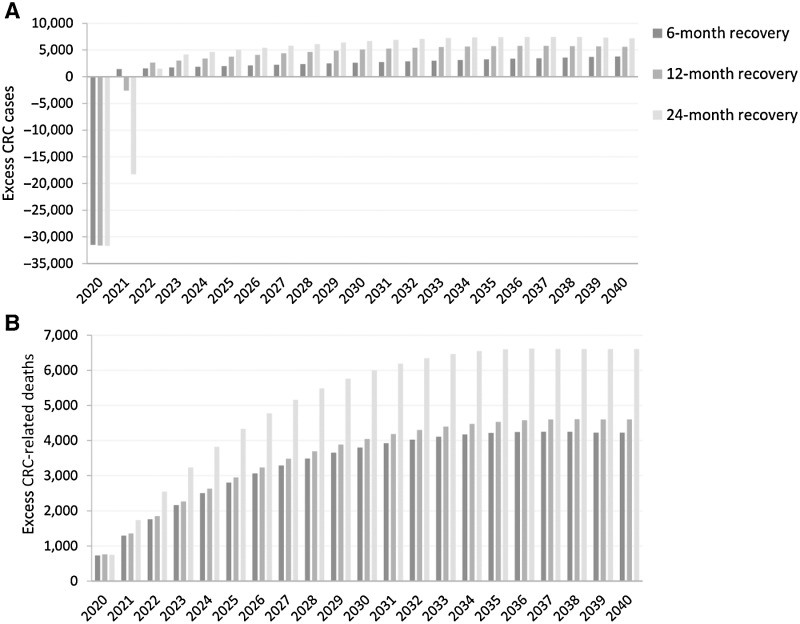
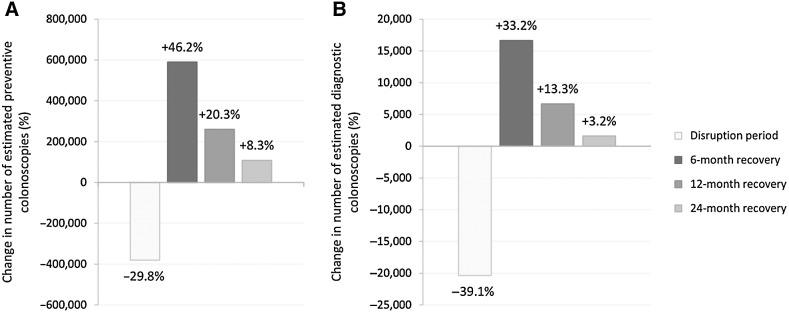
Methods: Using the MISCAN-Colon model, we simulated the US population and evaluated different impact and recovery scenarios. Scenarios were defined by the duration and severity of the disruption (percentage of eligible adults affected), the length of delays, and the duration of the recovery. During recovery (6, 12 or 24 months), capacity was increased to catch up missed procedures. Primary outcomes were excess colorectal cancer cases and -related deaths, and additional colonoscopies required during recovery.
Results: With a 24-month recovery, the model predicted that the US population would develop 7,210 (0.18%) excess colorectal cancer cases during 2020-2040, and 6,950 (0.65%) excess colorectal cancer-related deaths, and require 108,500 (8.6%) additional colonoscopies per recovery month, compared with a no-disruption scenario. Shorter recovery periods of 6 and 12 months, respectively, decreased excess colorectal cancer-related deaths to 4,190 (0.39%) and 4,580 (0.43%), at the expense of 260,200-590,100 (20.7%-47.0%) additional colonoscopies per month.
Conclusions: The COVID-19 pandemic will likely cause more than 4,000 excess colorectal cancer-related deaths in the US, which could increase to more than 7,000 if recovery periods are longer.
Impact: Our results highlight that catching-up colorectal cancer-related services within 12 months provides a good balance between required resources and mitigation of the impact of the disruption on colorectal cancer-related deaths.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
- 1055-9965. doi: 10.1158/1055-9965.EPI-32-1-HI
References
-
- Centers for Medicare & Medicaid Services. CMS adult elective surgery and procedures recommendations. 2020. Available from:https://www.cms.gov/files/document/cms-non-emergent-elective-medical-rec....
-
- Mast C, Munoz del Rio A. Epic Health Research Network . Delayed cancer screenings - a second look. 2020. Available from:https://epicresearch.org/articles/delayed-cancer-screenings-a-second-look.
-
- Elflein L. Delayed or cancelled routine cancer screening tests due to COVID-19 in the U.S. 2020. Available from:https://www.statista.com/statistics/1186490/delayed-cancelled-routine-ca....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
