

Adjusting growth standards for fetal sex improves correlation of small babies with stillbirth and adverse perinatal outcomes: A state-wide population study
- PMID: 36215239
- PMCID: PMC9551630
- DOI: 10.1371/journal.pone.0274521
Adjusting growth standards for fetal sex improves correlation of small babies with stillbirth and adverse perinatal outcomes: A state-wide population study
Abstract
Objectives: Sex impacts birthweight, with male babies heavier on average. Birthweight charts are thus sex specific, but ultrasound fetal weights are often reported by sex neutral standards. We aimed to identify what proportion of infants would be re-classified as SGA if sex-specific charts were used, and if this had a measurable impact on perinatal outcomes.
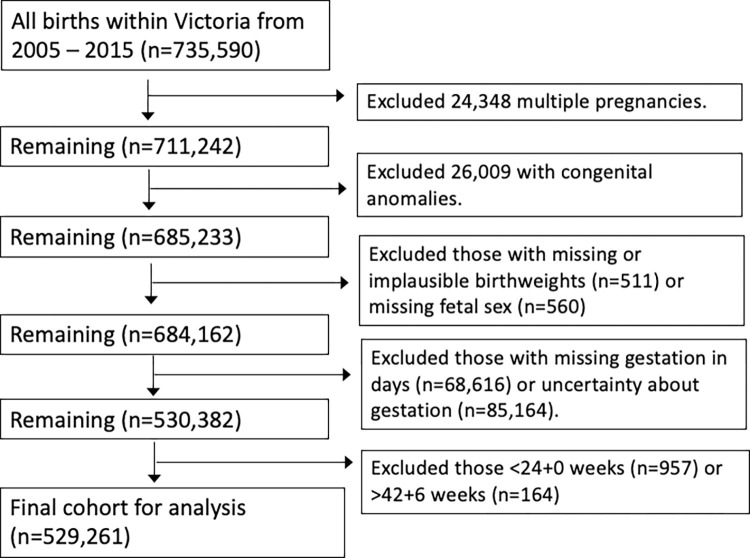
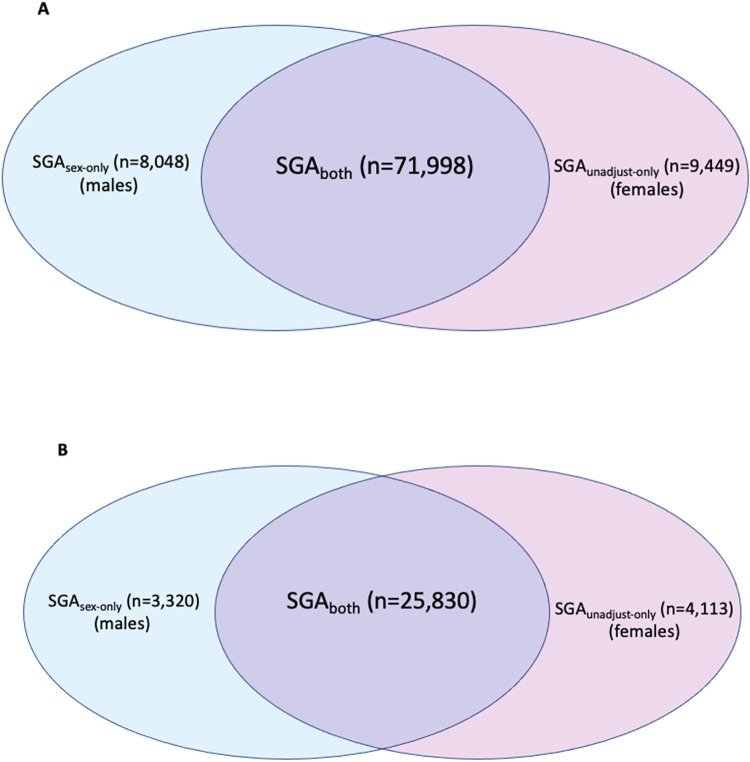
Methods: Retrospective cohort study including all infants born in Victoria, Australia, from 2005-2015 (529,261 cases). We applied GROW centiles, either adjusted or not adjusted for fetal sex. We compared overall SGA populations, and the populations of males considered small by sex-specific charts only (SGAsex-only), and females considered small by sex-neutral charts only (SGAunadjust-only).
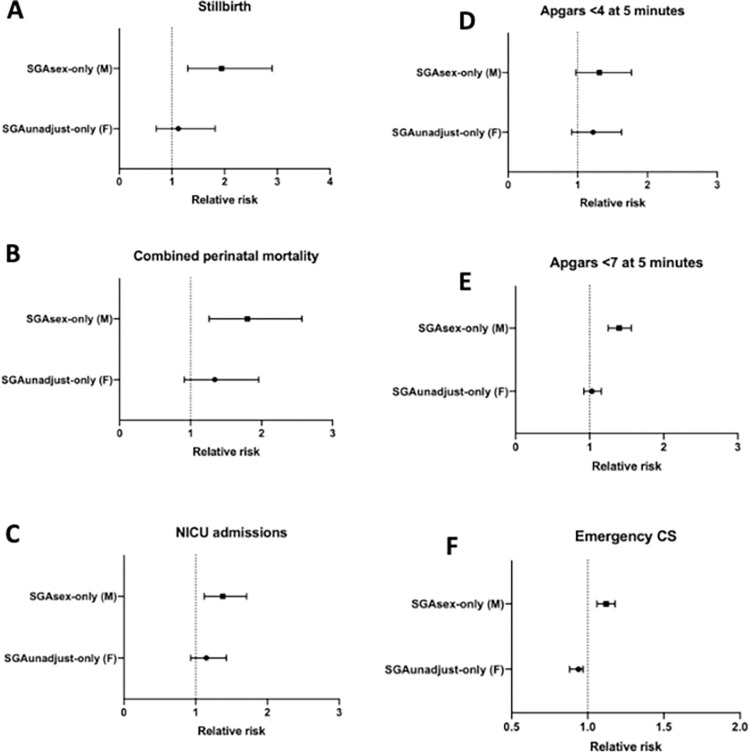
Results: Of those <10th centile by sex-neutral charts, 39.6% were male and 60.5% female, but using sex-specific charts, 50.3% were male and 49.7% female. 19.2% of SGA females were reclassified as average for gestational age (AGA) using sex-specific charts. These female newborns were not at increased risk of stillbirth, combined perinatal mortality, NICU admissions, low Apgars or emergency CS compared with an AGA infant, but were at greater risk of being iatrogenically delivered on suspicion of growth restriction. 25.0% male infants were reclassified as SGA by sex-specific charts. These male newborns, compared to the AGAall infant, were at greater risk of stillbirth (RR 1.94, 95%CI 1.30-2.90), combined perinatal mortality (RR 1.80, 95%CI 1.26-2.57), NICU admissions (RR 1.38, 95%CI 1.12-1.71), Apgars <7 at 5 minutes (RR 1.40, 95%CI 1.25-1.56) and emergency CS (RR 1.12, 95%CI 1.06-1.18).
Conclusions: Use of growth centiles not adjusted for fetal sex disproportionately classifies female infants as SGA, increasing their risk of unnecessary intervention, and fails to identify a cohort of male infants at increased risk of adverse outcomes, including stillbirth. Sex-specific charts may help inform decisions and improve outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Identification of the optimal growth charts for use in a preterm population: An Australian state-wide retrospective cohort study.PLoS Med. 2019 Oct 4;16(10):e1002923. doi: 10.1371/journal.pmed.1002923. eCollection 2019 Oct. PLoS Med. 2019. PMID: 31584941 Free PMC article.
-
Fetal size classified using gestational days rather than gestational weeks improves correlation with stillbirth risk: A statewide population study.PLoS One. 2022 Aug 10;17(8):e0271538. doi: 10.1371/journal.pone.0271538. eCollection 2022. PLoS One. 2022. PMID: 35947552 Free PMC article.
-
INTERGROWTH-21st compared with GROW customized centiles in the detection of adverse perinatal outcomes at term.J Matern Fetal Neonatal Med. 2020 Mar;33(6):961-966. doi: 10.1080/14767058.2018.1511696. Epub 2018 Oct 29. J Matern Fetal Neonatal Med. 2020. PMID: 30372647
-
Risk of stillbirth, preterm delivery, and fetal growth restriction following exposure in a previous birth: systematic review and meta-analysis.BJOG. 2018 Jan;125(2):183-192. doi: 10.1111/1471-0528.14906. Epub 2017 Oct 3. BJOG. 2018. PMID: 28856792
-
Preventing term stillbirth: benefits and limitations of using fetal growth reference charts.Curr Opin Obstet Gynecol. 2019 Dec;31(6):365-374. doi: 10.1097/GCO.0000000000000576. Curr Opin Obstet Gynecol. 2019. PMID: 31634162 Review.
Cited by
-
The Fetal Region-specific Optimized Growth Standard (FROGS)-A fetal and birthweight centile calculator validated in a national population.PLoS Med. 2025 Jun 20;22(6):e1004634. doi: 10.1371/journal.pmed.1004634. eCollection 2025 Jun. PLoS Med. 2025. PMID: 40540533 Free PMC article.
References
-
- Kady S, Gardosi J. Perinatal mortality and fetal growth restriction. Best Practice & Research Clinical Obstetrics & Gynaecology. 2004;18(3):397–410. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
