

Comparison of 68Ga-PSMA-617 PET/CT and 68Ga-RM2 PET/CT in Patients with Localized Prostate Cancer Who Are Candidates for Radical Prostatectomy: A Prospective, Single-Arm, Single-Center, Phase II Study
- PMID: 36215569
- PMCID: PMC10071805
- DOI: 10.2967/jnumed.122.263889
Comparison of 68Ga-PSMA-617 PET/CT and 68Ga-RM2 PET/CT in Patients with Localized Prostate Cancer Who Are Candidates for Radical Prostatectomy: A Prospective, Single-Arm, Single-Center, Phase II Study
Abstract
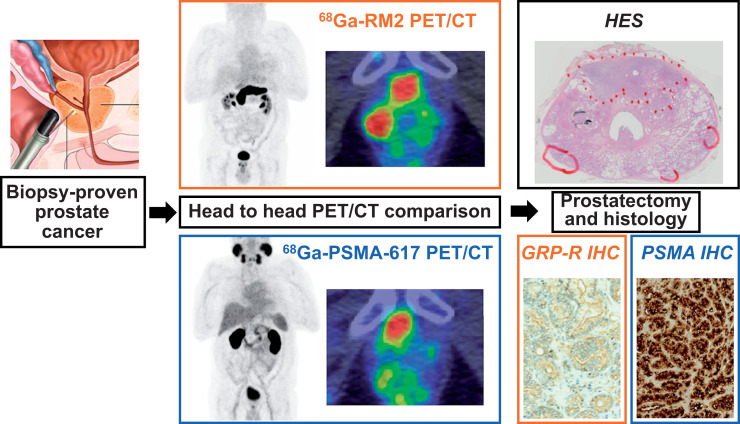
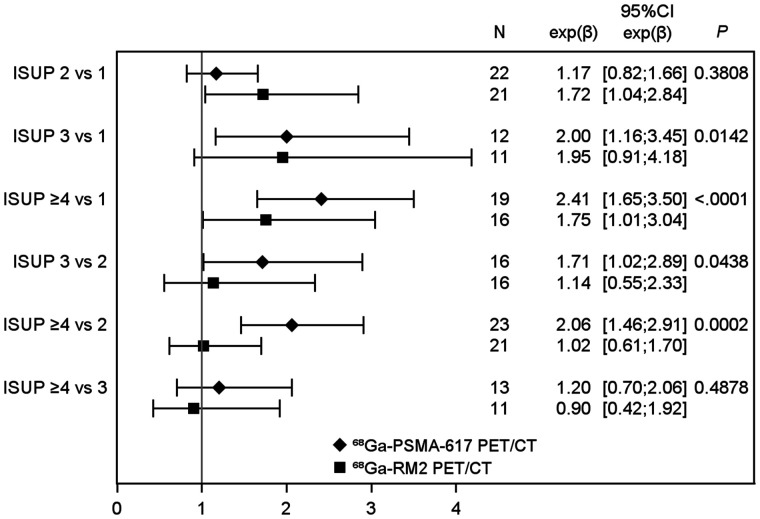
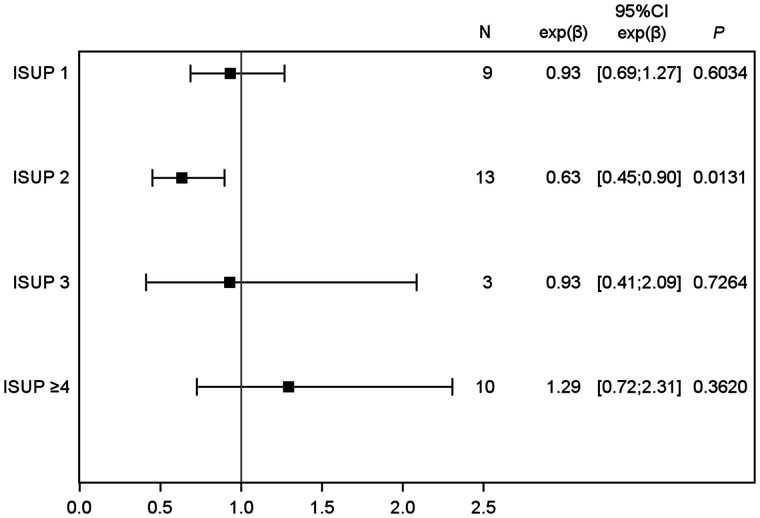
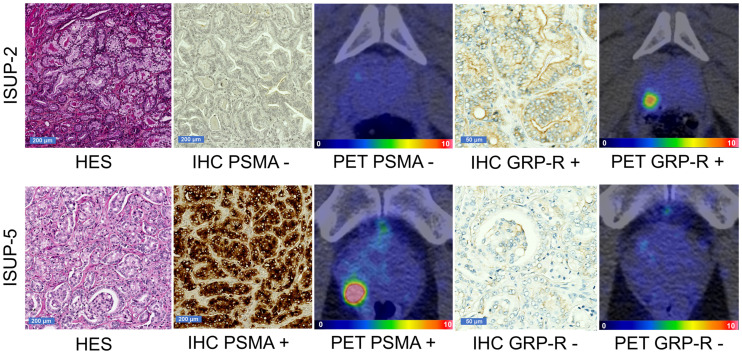
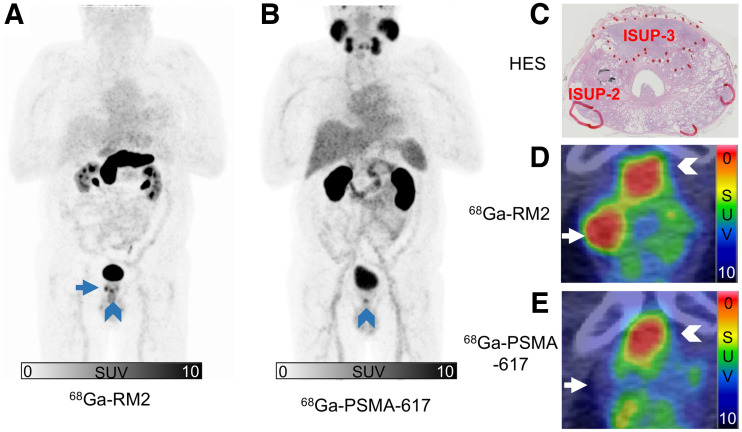
Considering the wide range of therapeutic options for localized prostate cancer (e.g., active surveillance, radiation-beam therapy, focal therapy, and radical prostatectomy), accurate assessment of the aggressiveness and localization of primary prostate cancer lesions is essential for treatment decision making. National Comprehensive Cancer Network guidelines recognize prostate-specific membrane antigen (PSMA) PET/CT for use in initial staging of high-risk primary prostate cancer. The gastrin-releasing peptide receptor (GRP-R) is a neuropeptide receptor overexpressed by low-risk prostate cancer cells. We aimed to perform the first (to our knowledge) prospective head-to-head comparison of PSMA- and GRP-R-targeted imaging at initial staging to understand how PSMA PET and GRP-R PET can be used or combined in clinical practice. Methods: This was a prospective, single-center, diagnostic cross-sectional imaging study using anonymized, masked, and independent interpretations of paired PET/CT studies in 22 patients with 68Ga-PSMA-617 (a radiolabeled PSMA inhibitor) and 68Ga-RM2 (68Ga-DOTA-4-amino-1-carboxymethylpiperidine-d-Phe-Gln-Trp-Ala-Val-Gly-His-Sta-Leu-NH2, a radiolabeled GRP-R antagonist). We enrolled patients with newly diagnosed, biopsy-proven prostate cancer. None had received neoadjuvant hormone therapy or chemotherapy, and all underwent extended pelvic lymph node dissection. Histologic findings served as a reference. Results: On a lesion-based analysis (including lesions < 0.1 cm3), 68Ga-PSMA-617 PET/CT detected 74.3% (26/35) of all tumor lesions and 68Ga-RM2 PET/CT detected 78.1% (25/32; 1 patient could not be offered 68Ga-RM2 PET/CT). Paired examinations showed positive uptake of the 2 tracers in 21 of 32 lesions (65.6%), negative uptake in 5 of 32 lesions (15.6%), and discordant uptake in 6 of 32 lesions (18.8%). Uptake of 68Ga-PSMA-617 was higher when the International Society of Urological Pathology (ISUP) score was at least 4 versus at least 1 (P < 0.0001) or 2 (P = 0.0002). There were no significant differences in uptake between ISUP scores for 68Ga-RM2. Median 68Ga-RM2 SUVmax was significantly higher than median 68Ga-PSMA-617 SUVmax in the ISUP-2 subgroup (P = 0.01). Conclusion: 68Ga-PSMA-617 PET/CT is useful to depict higher, more clinically significant ISUP score lesions, and 68Ga-RM2 PET/CT has a higher detection rate for low-ISUP tumors. Combining PSMA PET and GRP-R PET allows for better classification of intraprostatic lesions.
Keywords: GRP-R; PET; PSMA; imaging; prostate cancer.
© 2023 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67:7–30. - PubMed
-
- Schwarzenboeck SM, Rauscher I, Bluemel C, et al. . PSMA ligands for PET imaging of prostate cancer. J Nucl Med. 2017;58:1545–1552. - PubMed
-
- Uprimny C, Kroiss AS, Decristoforo C, et al. . 68Ga-PSMA-11 PET/CT in primary staging of prostate cancer: PSA and Gleason score predict the intensity of tracer accumulation in the primary tumour. Eur J Nucl Med Mol Imaging. 2017;44:941–949. - PubMed
-
- Acute lymphoblastic leukemia. National Comprehensive Cancer Network website. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1459. Published 2022. Accessed December 5, 2022.
-
- Mansi R, Fleischmann A, Mäcke HR, Reubi JC. Targeting GRPR in urological cancers: from basic research to clinical application. Nat Rev Urol. 2013;10:235–244. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous