

Physiological Bases for the Superiority of Apolipoprotein B Over Low-Density Lipoprotein Cholesterol and Non-High-Density Lipoprotein Cholesterol as a Marker of Cardiovascular Risk
- PMID: 36216435
- PMCID: PMC9673669
- DOI: 10.1161/JAHA.122.025858
Physiological Bases for the Superiority of Apolipoprotein B Over Low-Density Lipoprotein Cholesterol and Non-High-Density Lipoprotein Cholesterol as a Marker of Cardiovascular Risk
Abstract
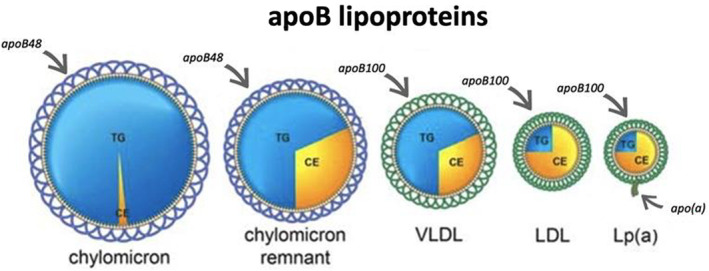
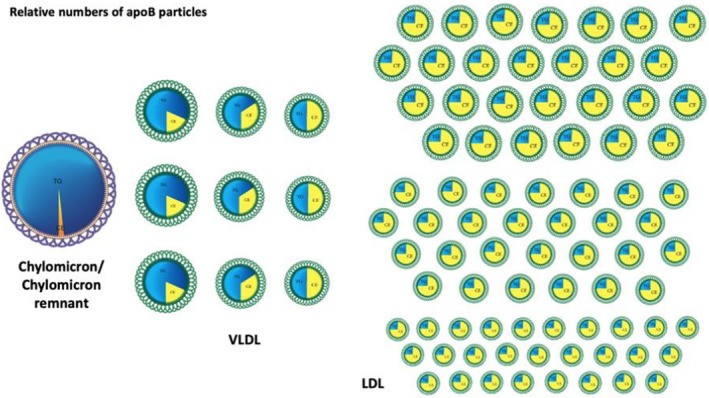
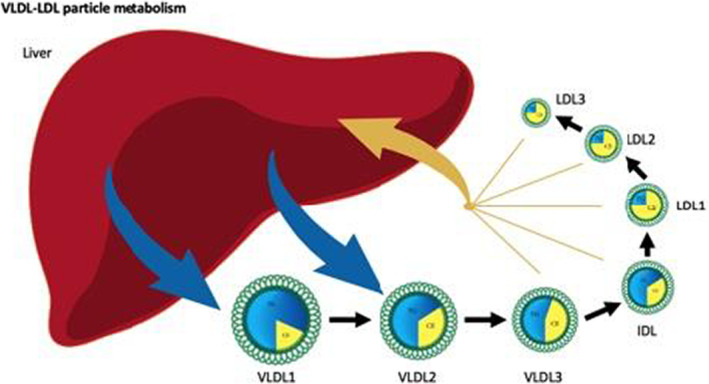
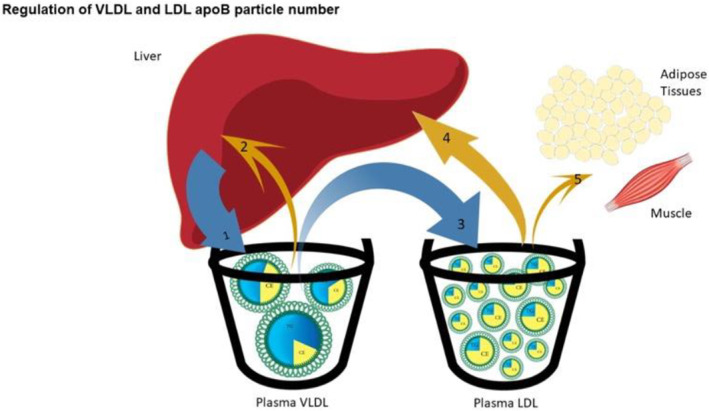
In 2019, the European Society of Cardiology/European Atherosclerosis Society stated that apolipoprotein B (apoB) was a more accurate marker of cardiovascular risk than low-density lipoprotein cholesterol (LDL-C) and non-high-density lipoprotein cholesterol. Since then, the evidence has continued to mount in favor of apoB. This review explicates the physiological mechanisms responsible for the superiority of apoB as a marker of the cardiovascular risk attributable to the atherogenic apoB lipoprotein particles chylomicron remnants, very low-density lipoprotein, and low-density lipoprotein particles. First, the nature and relative numbers of these different apoB particles will be outlined. This will make clear why low-density lipoprotein particles are almost always the major determinants of cardiovascular risk and why the concentrations of triglycerides and LDL-C may obscure this relation. Next, the mechanisms that govern the number of very low-density lipoprotein and low-density lipoprotein particles will be outlined because, except for dysbetalipoproteinemia, the total number of apoB particles determines cardiovascular risk, Then, the mechanisms that govern the cholesterol mass within very low-density lipoprotein and low-density lipoprotein particles will be reviewed because these are responsible for the discordance between the mass of cholesterol within apoB particles, measured either as LDL-C or non-high-density lipoprotein cholesterol, and the number of apoB particles measured as apoB, which creates the superior predictive power of apoB over LDL-C and non-high-density lipoprotein cholesterol. Finally, the major apoB dyslipoproteinemias will be briefly outlined. Our objective is to provide a physiological framework for health care givers to understand why apoB is a more accurate marker of cardiovascular risk than LDL-C or non-high-density lipoprotein cholesterol.
Keywords: apoB; apolipoprotein B; cardiovascular disease prevention; cardiovascular risk.
Figures
References
-
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, Chapman MJ, De Backer GG, Delgado V, Ference BA, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41:111–188. doi: 10.1093/eurheartj/ehz455 - DOI - PubMed
-
- Sniderman AD, Navar AM, Thanassoulis G. Apolipoprotein B vs low‐density lipoprotein cholesterol and non‐high‐density lipoprotein cholesterol as the primary measure of apolipoprotein B lipoprotein‐related risk: the debate is over. JAMA Cardiol. 2022;7:257–258. doi: 10.1001/jamacardio.2021.5080 - DOI - PubMed
-
- Richardson TG, Sanderson E, Palmer TM, Ala‐Korpela M, Ference BA, Davey Smith G, Holmes MV Rader DJ, ed. Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: a multivariable Mendelian randomisation analysis, PLoS Med. 2020;17:e1003062, doi: 10.1371/journal.pmed.1003062. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
