

Specific disruption of the ventral anterior temporo-frontal network reveals key implications for language comprehension and cognition
- PMID: 36217017
- PMCID: PMC9551096
- DOI: 10.1038/s42003-022-03983-9
Specific disruption of the ventral anterior temporo-frontal network reveals key implications for language comprehension and cognition
Abstract
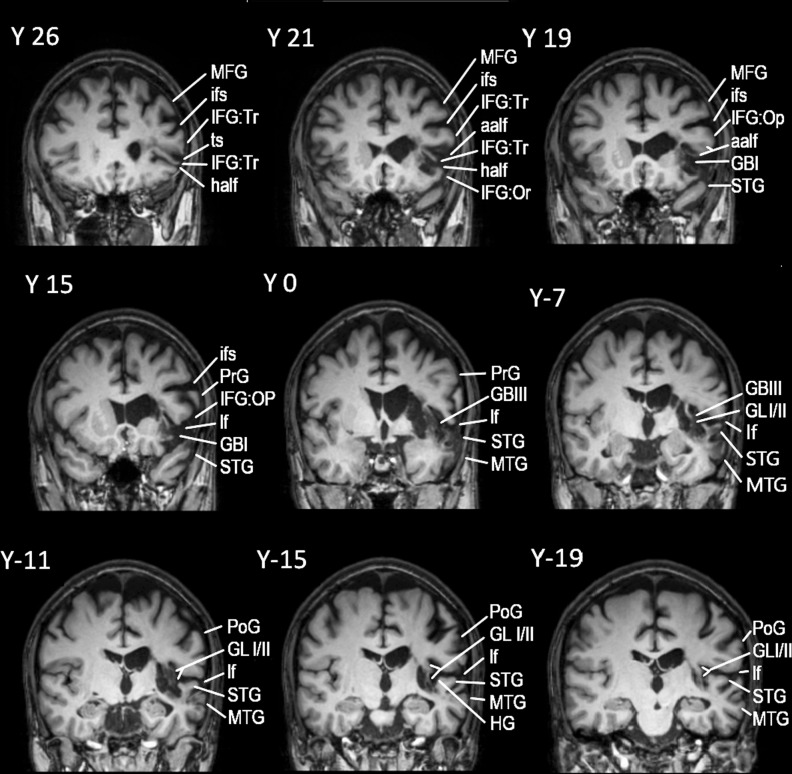
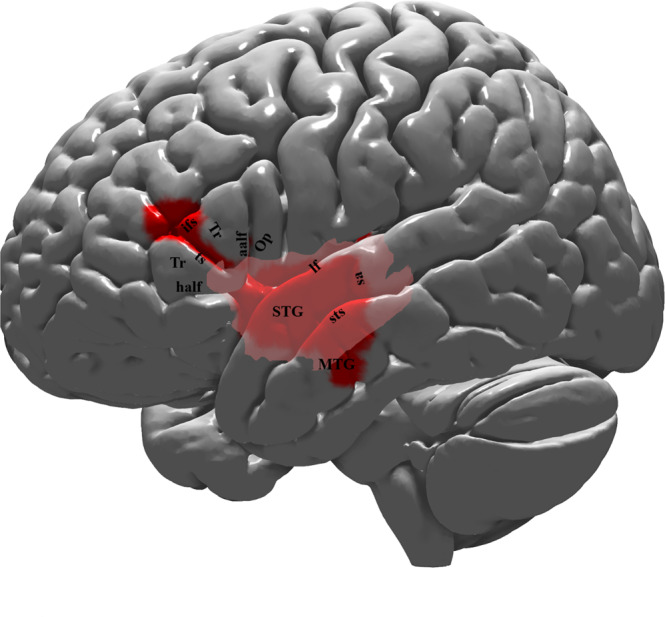
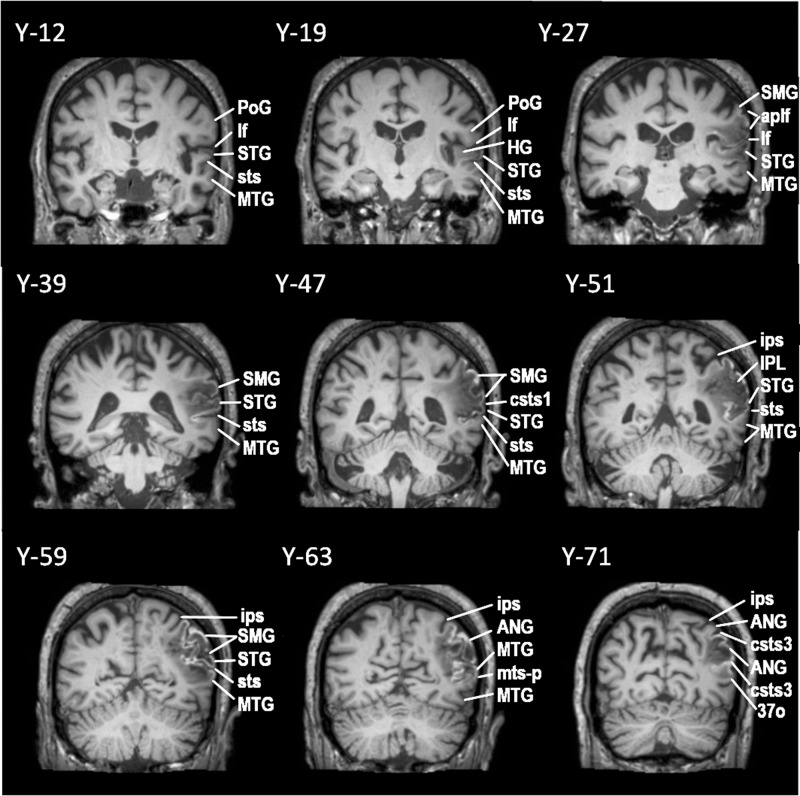
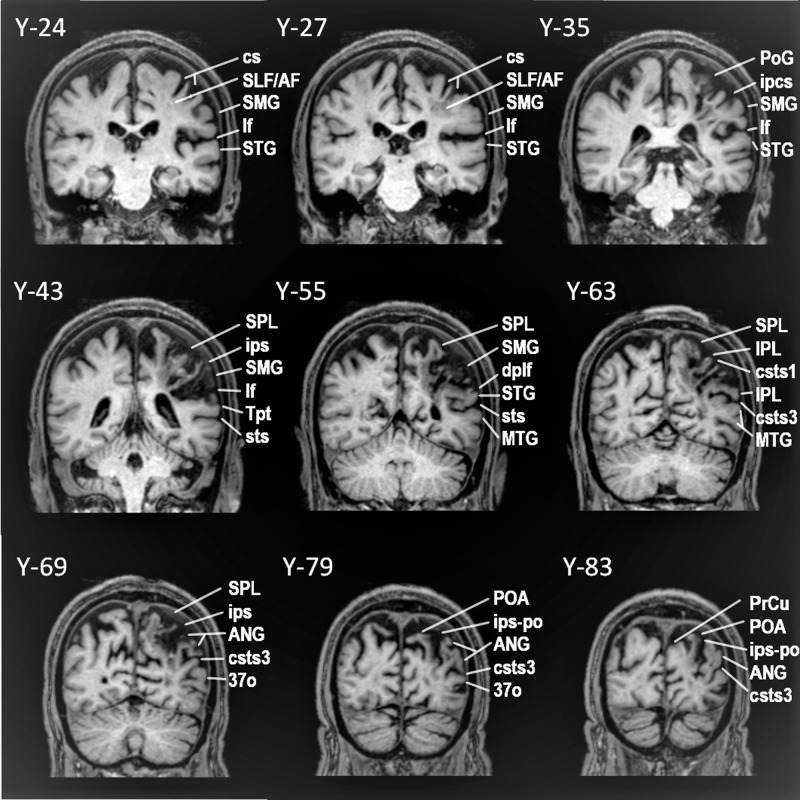
Recent investigations have raised the question of the role of the anterior lateral temporal cortex in language processing (ventral language network). Here we present the language and overall cognitive performance of a rare male patient with chronic middle cerebral artery cerebrovascular accident with a well-documented lesion restricted to the anterior temporal cortex and its connections via the extreme capsule with the pars triangularis of the inferior frontal gyrus (i.e. Broca's region). The performance of this unique patient is compared with that of two chronic middle cerebral artery cerebrovascular accident male patients with damage to the classic dorsal posterior temporo-parietal language system. Diffusion tensor imaging is used to reconstruct the relevant white matter tracts of the three patients, which are also compared with those of 10 healthy individuals. The patient with the anterior temporo-frontal lesion presents with flawless and fluent speech, but selective impairment in accessing lexico-semantic information, in sharp contrast to the impairments in speech, sentence comprehension and repetition observed after lesions to the classic dorsal language system. The present results underline the contribution of the ventral language stream in lexico-semantic processing and higher cognitive functions, such as active selective controlled retrieval.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
