

Risk Factors for Nephrotoxicity in Methicillin-Resistant Staphylococcus aureus Bacteraemia: A Post Hoc Analysis of the CAMERA2 Trial
- PMID: 36217068
- PMCID: PMC9834357
- DOI: 10.1007/s40261-022-01204-z
Risk Factors for Nephrotoxicity in Methicillin-Resistant Staphylococcus aureus Bacteraemia: A Post Hoc Analysis of the CAMERA2 Trial
Erratum in
-
Correction to: Risk Factors for Nephrotoxicity in Methicillin-Resistant Staphylococcus aureus Bacteraemia: A Post Hoc Analysis of the CAMERA2 Trial.Clin Drug Investig. 2023 Jan;43(1):35. doi: 10.1007/s40261-022-01224-9. Clin Drug Investig. 2023. PMID: 36401785 Free PMC article. No abstract available.
Abstract
Background: Clinical risk factors for nephrotoxicity in Staphylococcus aureus bacteraemia remain largely undetermined, despite its common occurrence and clinical significance. In an international, multicentre, prospective clinical trial (CAMERA2), which compared standard therapy (vancomycin monotherapy) to combination therapy (adding an anti-staphylococcal beta-lactam) for methicillin-resistant S. aureus bacteraemia, significantly more people in the combination therapy arm experienced acute kidney injury compared with those in the monotherapy arm (23% vs 6%).
Objective: The aim of this post hoc analysis was to explore in greater depth the risk factors for acute kidney injury from the CAMERA2 trial.
Methods: Among participants of the CAMERA2 trial, demographic-related, infection-related and treatment-related risk factors were assessed for their relationship with acute kidney injury by univariable and multivariable logistic regression. Acute kidney injury was defined by a modified-KDIGO (Kidney Disease: Improving Global Outcomes) criteria (not including urinary output).
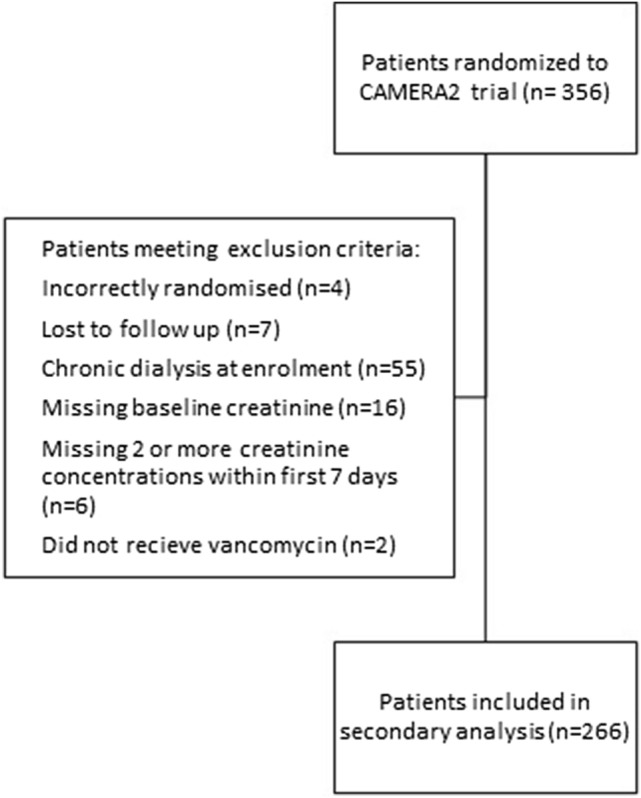
Results: Of the 266 participants included, age (p = 0.04), randomisation to combination therapy (p = 0.002), vancomycin area under the concentration-time curve (p = 0.03) and receipt of (flu)cloxacillin as the companion beta-lactam (p < 0.001) were significantly associated with acute kidney injury. On a multivariable analysis, concurrent use of (flu)cloxacillin increased the risk of acute kidney injury over four times compared with the use of cefazolin or no beta-lactam. The association of vancomycin area under the concentration-time curve with acute kidney injury also persisted in the multivariable model.
Conclusions: For participants receiving vancomycin for S. aureus bacteraemia, use of (flu)cloxacillin and increased vancomycin area under the concentration-time curve were risk factors for acute kidney injury. These represent potentially modifiable risk factors for nephrotoxicity and highlight the importance of avoiding the use of concurrent nephrotoxins.
© 2022. Crown.
Conflict of interest statement
Marc H. Scheetz has ongoing research contracts with Nevakar and SuperTrans Medical as well as having filed patent US10688195B2. He is supported in part by the National Institute of Allergy and Infectious Diseases under award number R21-AI149026. Jason A. Roberts acknowledge funding from the Australian National Health and Medical Research Council for a Centre of Research Excellence (APP2007007) and an Investigator Grant (APP2009736) as well as an Advancing Queensland Clinical Fellowship. Amy Legg, Niamh Meagher, Sandra A. Johnson, Matthew A. Roberts, Alan Cass, Jane Davies, Joshua S. Davis and Steven Y.C. Tong have no conflicts of interest that are directly relevant to the content of this article.
References
-
- Australian Commission on Safety and Quality in Health Care (ACSQHC) AURA 2019: third Australian report on antimicrobial use and resistance in human health. Sydney: ACSQHC; 2019.
-
- Kourtis AP, Hatfield K, Baggs J, Mu Y, See I, Epson E, et al. Vital signs: epidemiology and recent trends in methicillin-resistant and in methicillin-susceptible Staphylococcus aureus bloodstream infections: United States. MMWR Morb Mortal Wkly Rep. 2019;68(9):214–219. doi: 10.15585/mmwr.mm6809e1. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
