

Effectiveness of rectal artesunate as pre-referral treatment for severe malaria in children under 5 years of age: a multi-country observational study
- PMID: 36217159
- PMCID: PMC9550309
- DOI: 10.1186/s12916-022-02541-8
Effectiveness of rectal artesunate as pre-referral treatment for severe malaria in children under 5 years of age: a multi-country observational study
Abstract
Background: To prevent child deaths from severe malaria, early parenteral treatment is essential. Yet, in remote rural areas, accessing facilities offering parenteral antimalarials may be difficult. A randomised controlled trial found pre-referral treatment with rectal artesunate (RAS) to reduce deaths and disability in children who arrived at a referral facility with delay. This study examined the effectiveness of pre-referral RAS treatment implemented through routine procedures of established community-based health care systems.
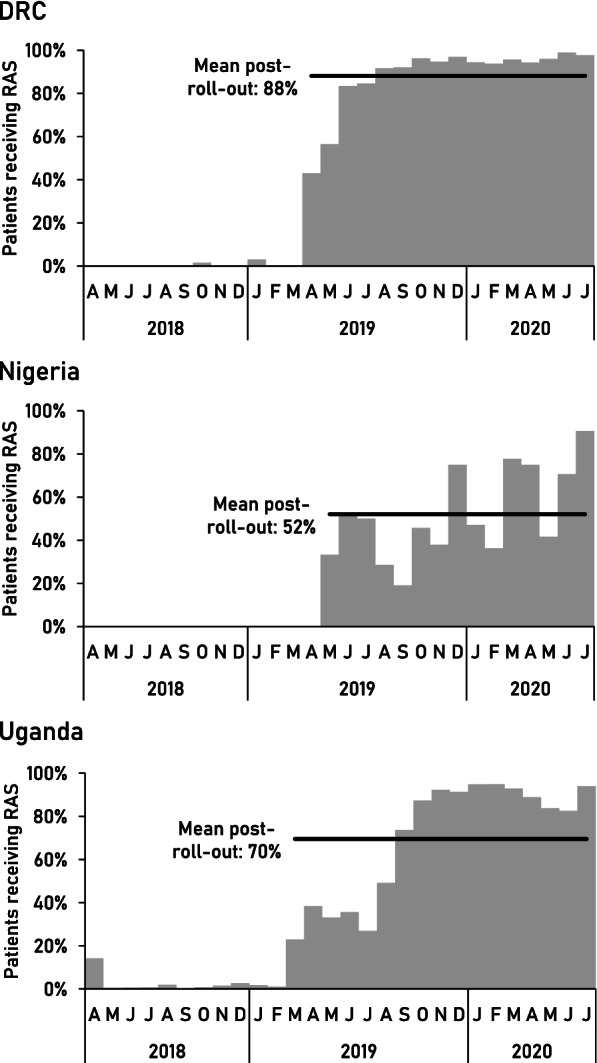
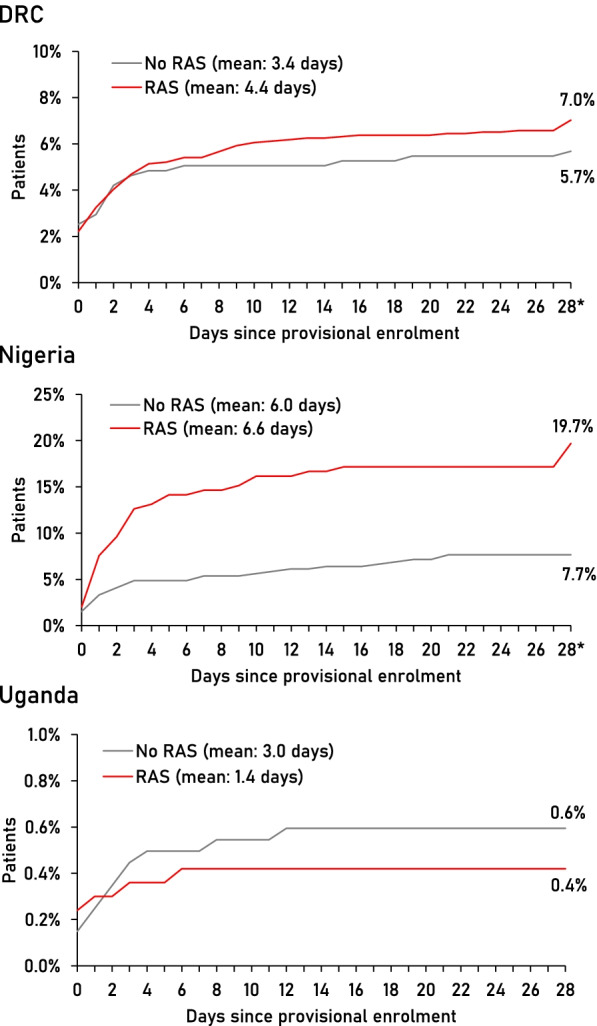
Methods: An observational study accompanied the roll-out of RAS in the Democratic Republic of the Congo (DRC), Nigeria and Uganda. Children <5 years of age presenting to a community-based health provider with a positive malaria test and signs of severe malaria were enrolled and followed up during admission and after 28 days to assess their health status and treatment history. The primary outcome was death; covariates of interest included RAS use, referral completion, and post-referral treatment.
Results: Post-roll-out, RAS was administered to 88% of patients in DRC, 52% in Nigeria, and 70% in Uganda. The overall case fatality rate (CFR) was 6.7% (135/2011) in DRC, 11.7% (69/589) in Nigeria, and 0.5% (19/3686) in Uganda; 13.8% (865/6286) of patients were sick on day 28. The CFR was higher after RAS roll-out in Nigeria (16.1 vs. 4.2%) and stable in DRC (6.7 vs. 6.6%) and Uganda (0.7 vs. 0.3%). In DRC and Nigeria, children receiving RAS were more likely to die than those not receiving RAS (aOR=3.06, 95% CI 1.35-6.92 and aOR=2.16, 95% CI 1.11-4.21, respectively). Only in Uganda, RAS users were less likely to be dead or sick at follow-up (aOR=0.60, 95% CI 0.45-0.79). Post-referral parenteral antimalarials plus oral artemisinin-based combination therapy (ACT), a proxy for appropriate post-referral treatment, was protective. However, in referral health facilities, ACT was not consistently administered after parenteral treatment (DRC 68.4%, Nigeria 0%, Uganda 70.9%).
Conclusions: Implemented at scale to the recommended target group, pre-referral RAS had no beneficial effect on child survival in three highly malaria-endemic settings. RAS is unlikely to reduce malaria deaths unless health system issues such as referral and quality of care at all levels are addressed.
Trial registration: The study is registered on ClinicalTrials.gov : NCT03568344.
Keywords: Case management; Child mortality; Community health worker; Malaria mortality; Malaria treatment; Rectal artesunate; Referral; Severe malaria.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Comment in
-
Pre-referral rectal artesunate is no "magic bullet" in weak health systems.BMC Med. 2023 Mar 30;21(1):119. doi: 10.1186/s12916-023-02777-y. BMC Med. 2023. PMID: 36991404 Free PMC article.
-
The CARAMAL study could not assess the effectiveness of rectal artesunate in treating suspected severe malaria.BMC Med. 2023 Mar 30;21(1):118. doi: 10.1186/s12916-023-02776-z. BMC Med. 2023. PMID: 36991487 Free PMC article.
References
-
- World Health Organization . World Malaria Report 2021. Geneva: World Health Organization; 2021.
-
- World Health Organization . Guidelines for the treatment of malaria. 3. Geneva: World Health Organization; 2015. - PubMed
-
- Young M, Wolfheim C, Marsh DR, Hammamy D. World Health Organization/United Nations Children's Fund Joint Statement on Integrated Community Case Management: An Equity-Focused Strategy to Improve Access to Essential Treatment Services for Children. Am Soc Trop Med Hyg. 2012;87(5_Suppl):6–10. doi: 10.4269/ajtmh.2012.12-0221. - DOI - PMC - PubMed
-
- Karra M, Fink G, Canning D. Facility distance and child mortality: a multi-country study of health facility access, service utilization, and child health outcomes. Int J Epidemiol. 2017;46(3):817–826. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
