

Contribution of coronal vertebral and IVD wedging to Cobb angle changes in adolescent idiopathic scoliosis during growth
- PMID: 36217198
- PMCID: PMC9549629
- DOI: 10.1186/s12891-022-05863-z
Contribution of coronal vertebral and IVD wedging to Cobb angle changes in adolescent idiopathic scoliosis during growth
Abstract
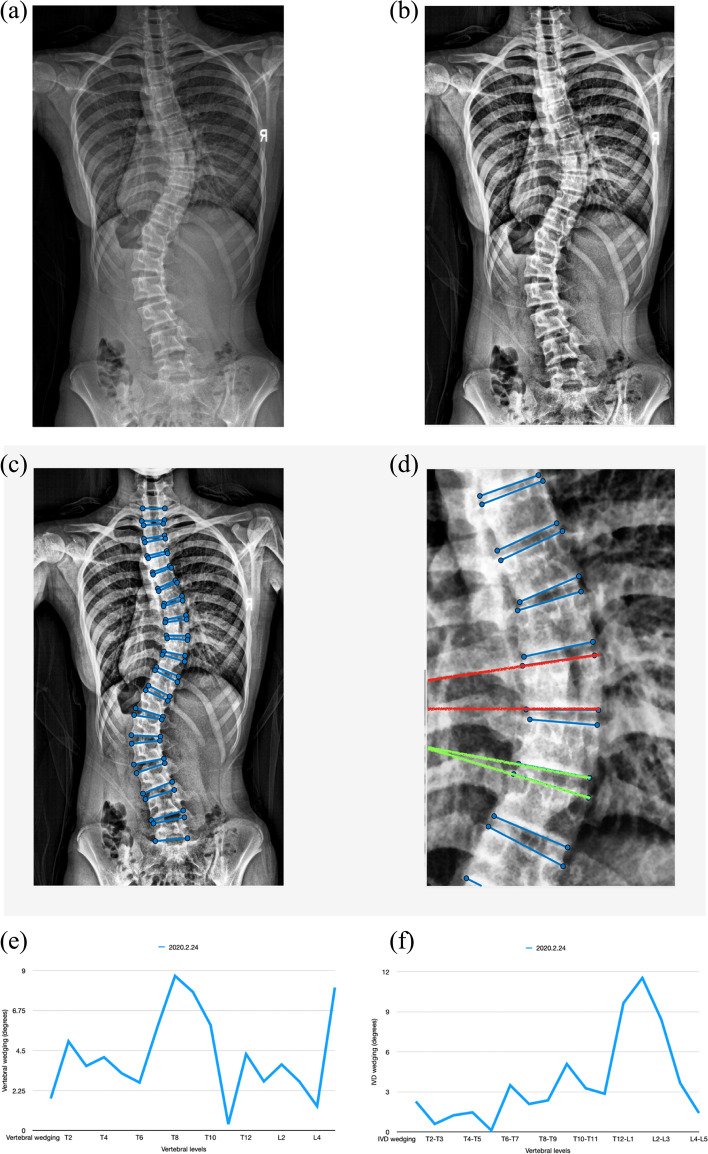
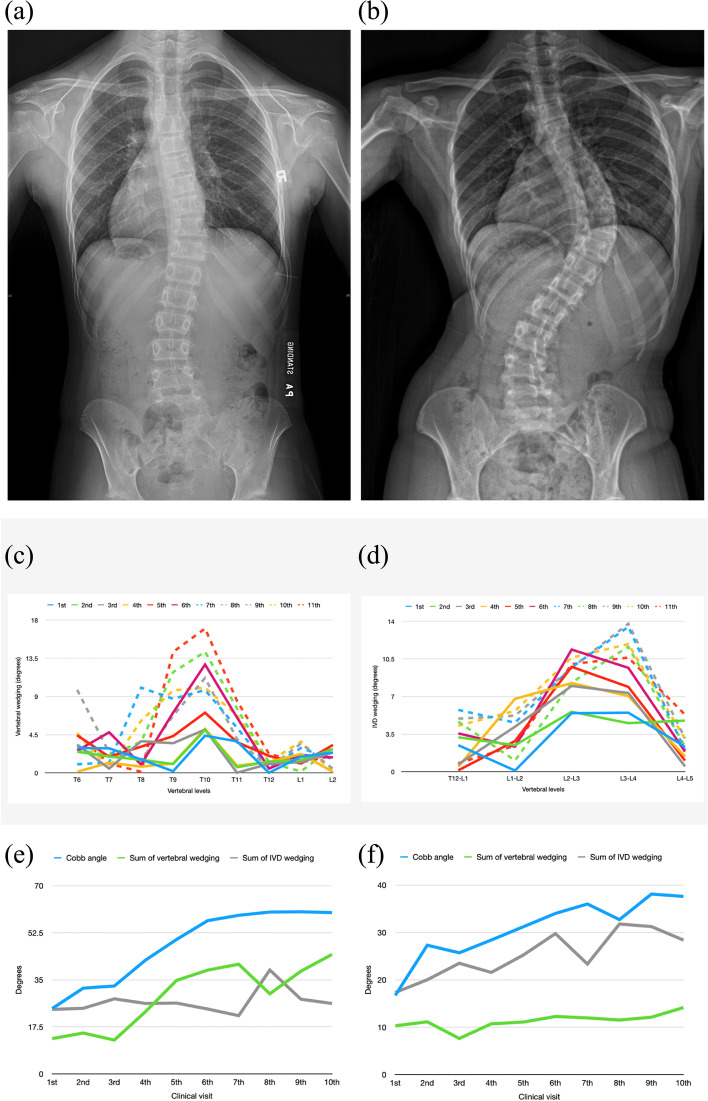
Study design: Prospective study BACKGROUND: Vertebral and intervertebral disc (IVD) wedging are often seen in patients with adolescent idiopathic scoliosis (AIS). However, the relationship between wedging and curve progression, and the change of wedging before bracing to final weaning is unknown. The aim of this study was to investigate the pattern and sequence of vertebral and IVD wedging development, and to determine the relationship between the change of wedging and curve progression in AIS during growth.
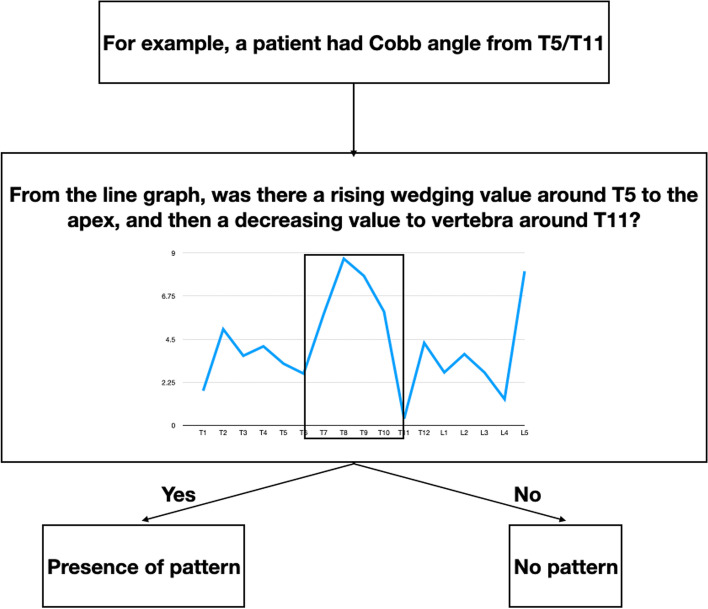
Methods: This was a prospective study of 32 AIS females with right-sided thoracic curves and/or left-sided lumbar curves who completed brace treatment. They were classified into progression and non-progression groups. Vertebral and IVD wedging were calculated for each spinal segment. The wedging pattern was first identified and then used to determine the sequence of wedging development. Percentage change in the sum of wedging during growth was calculated and compared.
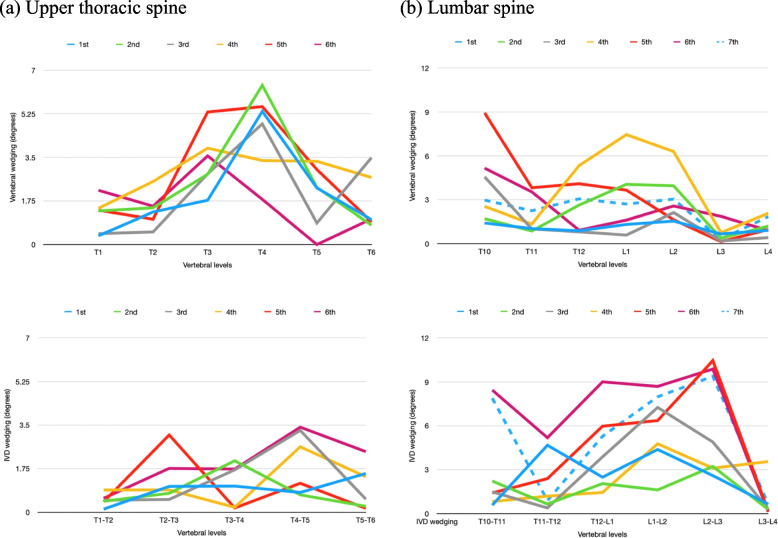
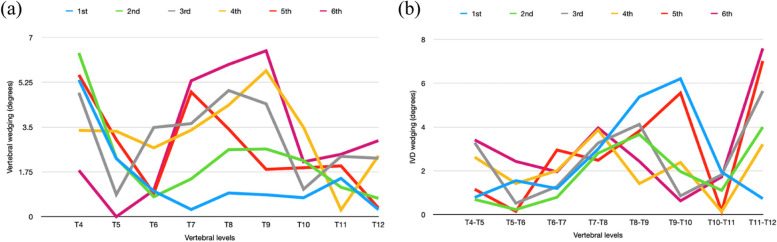
Results: The sum of vertebral wedging for both groups was 2.4° to 8.7° more than that of IVD wedging in the thoracic spine but 8.7° to 17.7° less in the lumbar spine. Out of the 20 curves assessed, 5 thoracic curves and 1 lumbar curve developed vertebral wedging before IVD wedging, and 3 thoracic curves and 4 lumbar curves had the opposite pattern. The progression group had larger increases in sum of vertebral (40%) and IVD (28.6%) wedging as compared to the non-progression group (both 16.7%). A significant difference in wedging between the first and the latest visits was found in the progression group only (p < 0.05).
Conclusion: Pattern and sequence of vertebral and IVD wedging were related to the location of the curve rather than the presence of curve progression. Progressed curves were associated with increased wedging during growth.
Level of evidence: II.
Keywords: Adolescent idiopathic scoliosis; Deformity; Disc; Wedging.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





Similar articles
-
Sequential MRI reveals vertebral body wedging significantly contributes to coronal plane deformity progression in adolescent idiopathic scoliosis during growth.Spine Deform. 2020 Oct;8(5):901-910. doi: 10.1007/s43390-020-00138-w. Epub 2020 May 25. Spine Deform. 2020. PMID: 32451976
-
Comparison of disc and vertebral wedging between patients with adolescent idiopathic scoliosis and Chiari malformation-associated scoliosis.J Spinal Disord Tech. 2012 Jul;25(5):277-84. doi: 10.1097/BSD.0b013e31821f4f10. J Spinal Disord Tech. 2012. PMID: 21617568
-
The effectiveness of selective thoracic fusion for treating adolescent idiopathic scoliosis: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Nov;13(11):4-16. doi: 10.11124/jbisrir-2015-2338. JBI Database System Rev Implement Rep. 2015. PMID: 26657460
-
Curve type, flexibility, correction, and rotation are predictors of curve progression in patients with adolescent idiopathic scoliosis undergoing conservative treatment : a systematic review.Bone Joint J. 2022 Apr;104-B(4):424-432. doi: 10.1302/0301-620X.104B4.BJJ-2021-1677.R1. Bone Joint J. 2022. PMID: 35360948 Free PMC article.
-
The cartilage matrisome in adolescent idiopathic scoliosis.Bone Res. 2020 Mar 9;8:13. doi: 10.1038/s41413-020-0089-0. eCollection 2020. Bone Res. 2020. PMID: 32195011 Free PMC article. Review.
Cited by
-
Correlation between coronal wedge deformity and sagittal spinal curvature in adolescent idiopathic scoliosis: a retrospective analysis.Sci Rep. 2024 Nov 23;14(1):29038. doi: 10.1038/s41598-024-80704-8. Sci Rep. 2024. PMID: 39580533 Free PMC article.
-
Biomechanical analysis of spinal range of motion and intervertebral disc loadings in normal and adolescent idiopathic scoliosis models.Front Bioeng Biotechnol. 2025 Feb 19;13:1473776. doi: 10.3389/fbioe.2025.1473776. eCollection 2025. Front Bioeng Biotechnol. 2025. PMID: 40046810 Free PMC article.
-
Segmental deformity markers offer novel indicators of deformity progression risk in deformity-matched adolescent idiopathic scoliosis patients.Spine Deform. 2024 Nov;12(6):1647-1655. doi: 10.1007/s43390-024-00927-7. Epub 2024 Jul 24. Spine Deform. 2024. PMID: 39044108 Free PMC article.
-
3D prediction of curve progression in adolescent idiopathic scoliosis based on biplanar radiological reconstruction.Bone Jt Open. 2024 Mar 25;5(3):243-251. doi: 10.1302/2633-1462.53.BJO-2023-0176.R1. Bone Jt Open. 2024. PMID: 38522456 Free PMC article.
-
The single-cell transcription reveals the aberrant differentiation trajectory of chondrocytes in the intervertebral disc for congenital scoliosis.iScience. 2025 May 8;28(6):112608. doi: 10.1016/j.isci.2025.112608. eCollection 2025 Jun 20. iScience. 2025. PMID: 40502710 Free PMC article.
References
-
- Kuznia AL, Hernandez AK, Lee LU. Adolescent Idiopathic Scoliosis: Common Questions and Answers. Am Fam Physician. 2020;101(1):19. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
