

Alternative Complement Pathway Inhibition With Iptacopan for the Treatment of C3 Glomerulopathy-Study Design of the APPEAR-C3G Trial
- PMID: 36217526
- PMCID: PMC9546729
- DOI: 10.1016/j.ekir.2022.07.004
Alternative Complement Pathway Inhibition With Iptacopan for the Treatment of C3 Glomerulopathy-Study Design of the APPEAR-C3G Trial
Abstract
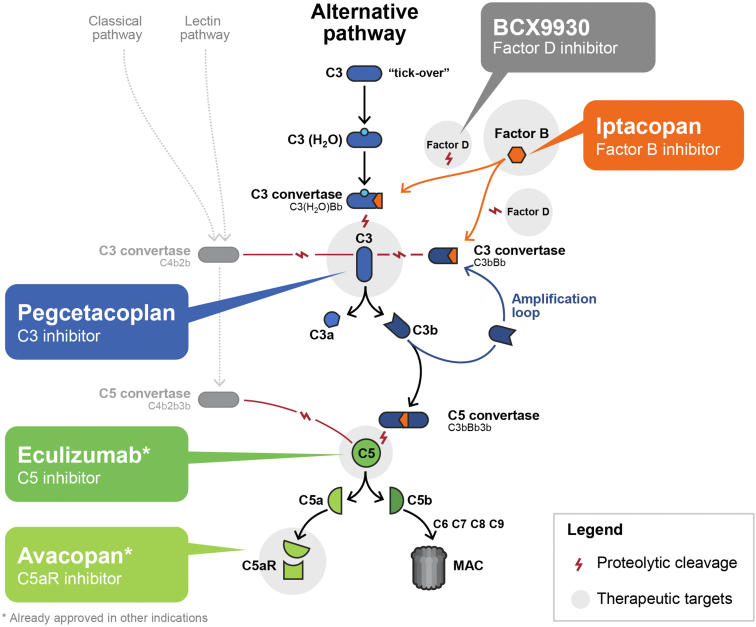
Introduction: Complement 3 glomerulopathy (C3G) is a rare kidney disease characterized by dysregulation of the alternative pathway (AP) of the complement system. About 50% of patients with C3G progress to kidney failure within 10 years of diagnosis. Currently, there are no approved therapeutic agents for C3G. Iptacopan is an oral, first-in-class, potent, and selective inhibitor of factor B, a key component of the AP. In a Phase II study, treatment with iptacopan was associated with a reduction in proteinuria and C3 deposit scores in C3G patients with native and transplanted kidneys, respectively.
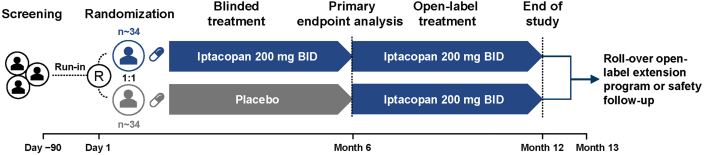
Methods: APPEAR-C3G (NCT04817618) is a randomized, double-blind, and placebo-controlled Phase III study to evaluate the efficacy and safety of iptacopan in C3G patients, enrolling 68 adults with biopsy-confirmed C3G, reduced C3 (<77 mg/dl), proteinuria ≥1.0 g/g, and estimated glomerular filtration rate (eGFR) ≥30 ml/min per 1.73 m2. All patients will receive maximally tolerated angiotensin-converting enzyme inhibitor/angiotensin receptor blocker and vaccination against encapsulated bacteria. Patients with any organ transplantation, progressive crescentic glomerulonephritis (GN), monoclonal gammopathy of undetermined significance, or kidney biopsy with >50% interstitial fibrosis/tubular atrophy, will be excluded. Patients will be randomized 1:1 to receive either iptacopan 200 mg twice daily or placebo for 6 months, followed by open-label treatment with iptacopan 200 mg twice daily for all patients for 6 months. The primary objective is to evaluate the efficacy of iptacopan versus placebo on proteinuria reduction urine protein:creatinine ratio (UPCR) (24 h urine). Key secondary endpoints will assess kidney function measured by eGFR, histological disease total activity score, and fatigue.
Conclusion: This study aims to demonstrate the clinical benefits of AP inhibition with iptacopan in C3G.
Keywords: C3G; LNP023; alternative pathway; clinical trials; complement system; factor B; iptacopan.
© 2022 International Society of Nephrology. Published by Elsevier Inc.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
