

TP53-Mutated Myelodysplastic Syndrome and Acute Myeloid Leukemia: Biology, Current Therapy, and Future Directions
- PMID: 36218325
- PMCID: PMC9627130
- DOI: 10.1158/2159-8290.CD-22-0332
TP53-Mutated Myelodysplastic Syndrome and Acute Myeloid Leukemia: Biology, Current Therapy, and Future Directions
Erratum in
-
Correction: TP53-Mutated Myelodysplastic Syndrome and Acute Myeloid Leukemia: Biology, Current Therapy, and Future Directions.Cancer Discov. 2022 Dec 2;12(12):2954. doi: 10.1158/2159-8290.CD-22-1192. Cancer Discov. 2022. PMID: 36458434 Free PMC article. No abstract available.
Abstract
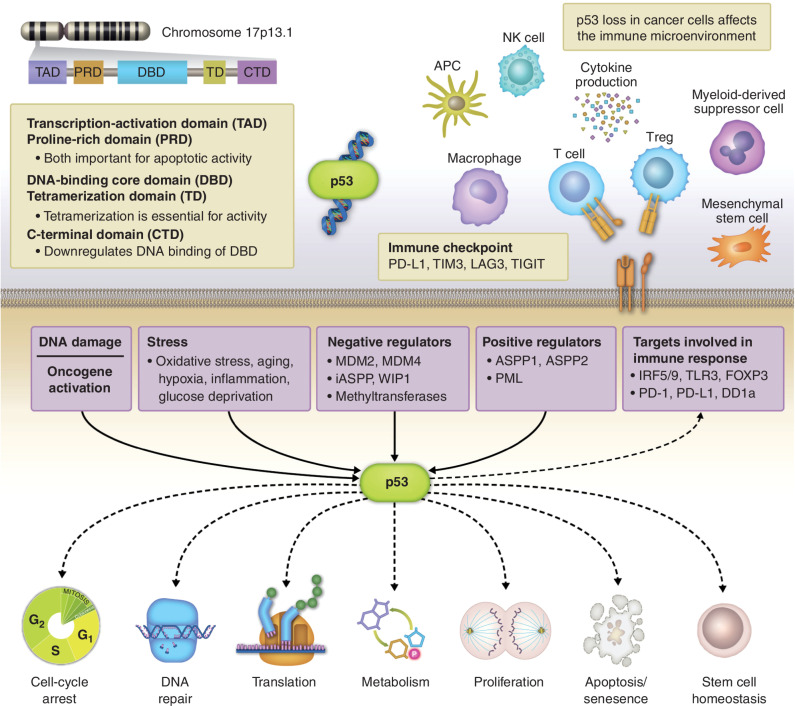
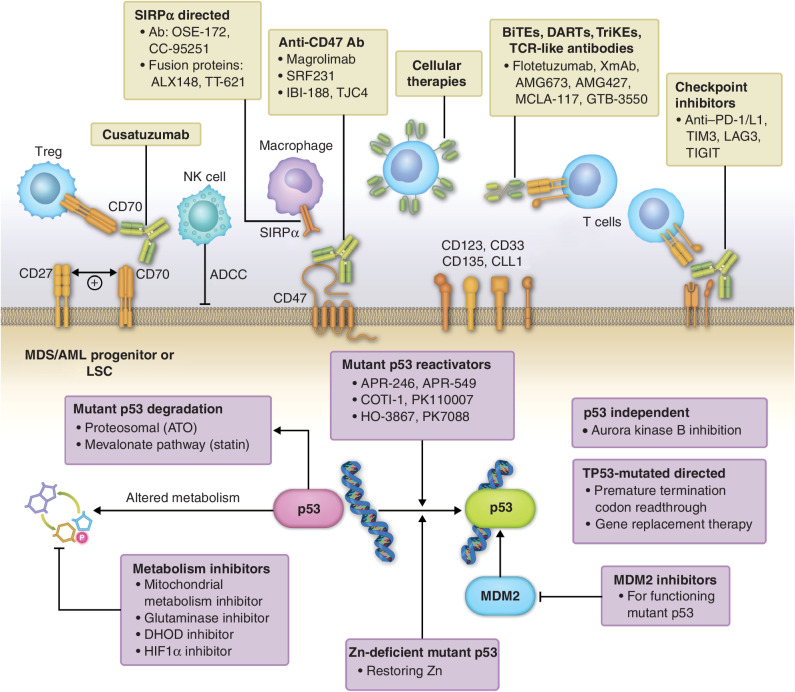
TP53-mutated myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML) form a distinct group of myeloid disorders with dismal outcomes. TP53-mutated MDS and AML have lower response rates to either induction chemotherapy, hypomethylating agent-based regimens, or venetoclax-based therapies compared with non-TP53-mutated counterparts and a poor median overall survival of 5 to 10 months. Recent advances have identified novel pathogenic mechanisms in TP53-mutated myeloid malignancies, which have the potential to improve treatment strategies in this distinct clinical subgroup. In this review, we discuss recent insights into the biology of TP53-mutated MDS/AML, current treatments, and emerging therapies, including immunotherapeutic and nonimmune-based approaches for this entity.
Significance: Emerging data on the impact of cytogenetic aberrations, TP53 allelic burden, immunobiology, and tumor microenvironment of TP53-mutated MDS and AML are further unraveling the complexity of this disease. An improved understanding of the functional consequences of TP53 mutations and immune dysregulation in TP53-mutated AML/MDS coupled with dismal outcomes has resulted in a shift from the use of cytotoxic and hypomethylating agent-based therapies to novel immune and nonimmune strategies for the treatment of this entity. It is hoped that these novel, rationally designed combinations will improve outcomes in this area of significant unmet need.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Sabapathy K, Lane DP. Therapeutic targeting of p53: all mutants are equal, but some mutants are more equal than others. Nat Rev Clin Oncol 2018;15:13–30. - PubMed
-
- Lakin ND, Jackson SP. Regulation of p53 in response to DNA damage. Oncogene 1999;18:7644–55. - PubMed
-
- Bowen D, Groves MJ, Burnett AK, Patel Y, Allen C, Green C, et al. TP53 gene mutation is frequent in patients with acute myeloid leukemia and complex karyotype, and is associated with very poor prognosis. Leukemia 2009;23:203–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
