

Home Blood Pressure Self-monitoring plus Self-titration of Antihypertensive Medication for Poorly Controlled Hypertension in Primary Care: the ADAMPA Randomized Clinical Trial
- PMID: 36219303
- PMCID: PMC9849508
- DOI: 10.1007/s11606-022-07791-z
Home Blood Pressure Self-monitoring plus Self-titration of Antihypertensive Medication for Poorly Controlled Hypertension in Primary Care: the ADAMPA Randomized Clinical Trial
Abstract
Background: Patient empowerment through pharmacological self-management is a common strategy in some chronic diseases such as diabetes, but it is rarely used for controlling blood pressure.
Objective: This study aimed to assess self-monitoring plus self-titration of antihypertensive medication versus usual care for reducing systolic blood pressure (SBP) at 12 months in poorly controlled hypertensive patients.
Design: The ADAMPA study was a pragmatic, controlled, randomized, non-masked clinical trial with two parallel arms in Valencia, Spain.
Participants: Hypertensive patients older than 40 years, with SBP over 145 mmHg and/or diastolic blood pressure (DBP) over 90 mmHg, were recruited from July 2017 to June 2018.
Intervention: Participants were randomized 1:1 to usual care versus an individualized, pre-arranged plan based on self-monitoring plus self-titration.
Main measure: The primary outcome was the adjusted mean difference (AMD) in SBP between groups at 12 months.
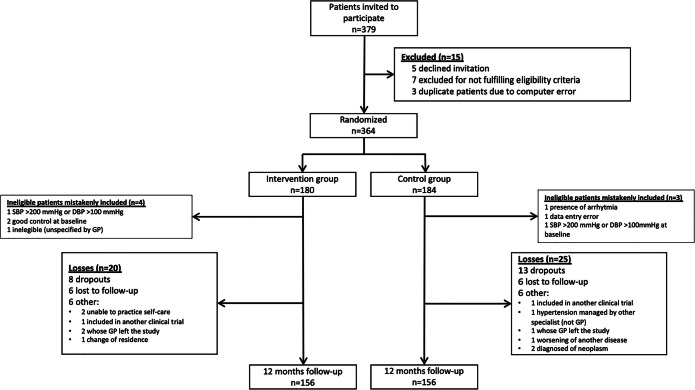
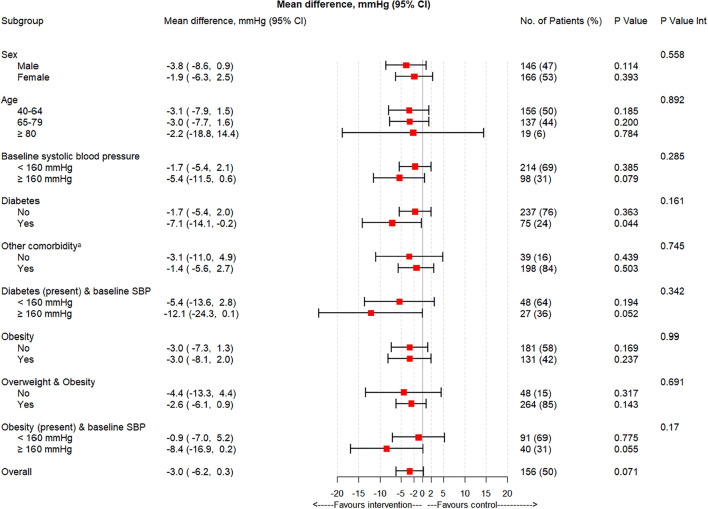
Key results: Primary outcome data were available for 312 patients (intervention n=156, control n=156) of the 366 who were initially recruited. The AMD in SBP at 12 months (main analysis) was -2.9 mmHg (95% CI, -5.9 to 0.1, p=0.061), while the AMD in DBP was -1.9 mmHg (95% CI, -3.7 to 0.0, p=0.052). The results of the subgroup analysis were consistent with these for the main outcome measures. More patients in the intervention group achieved good blood pressure control (<140/90 mmHg) at 12 months than in the control group (55.8% vs 42.3%, difference 13.5%, 95% CI, 2.5 to 24.5%, p=0.017). At 12 months, no differences were observed in behavior, quality of life, use of health services, or adverse events.
Conclusion: Self-monitoring plus self-titration of antihypertensive medication based on an individualized pre-arranged plan used in primary care may be a promising strategy for reducing blood pressure at 12 months compared to usual care, without increasing healthcare utilization or adverse events.
Trial registration: EudraCT, number 2016-003986-25 (registered 17 March 2017) and clinicaltrials.gov , NCT03242785.
Keywords: blood pressure self-management; blood pressure self-monitoring; patient empowerment; primary care; randomized clinical trial.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2224–60. doi: 10.1016/S0140-6736(12)61766-8. - DOI - PMC - PubMed
-
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1923-94. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
