

Artificial intelligence for multimodal data integration in oncology
- PMID: 36220072
- PMCID: PMC10655164
- DOI: 10.1016/j.ccell.2022.09.012
Artificial intelligence for multimodal data integration in oncology
Abstract
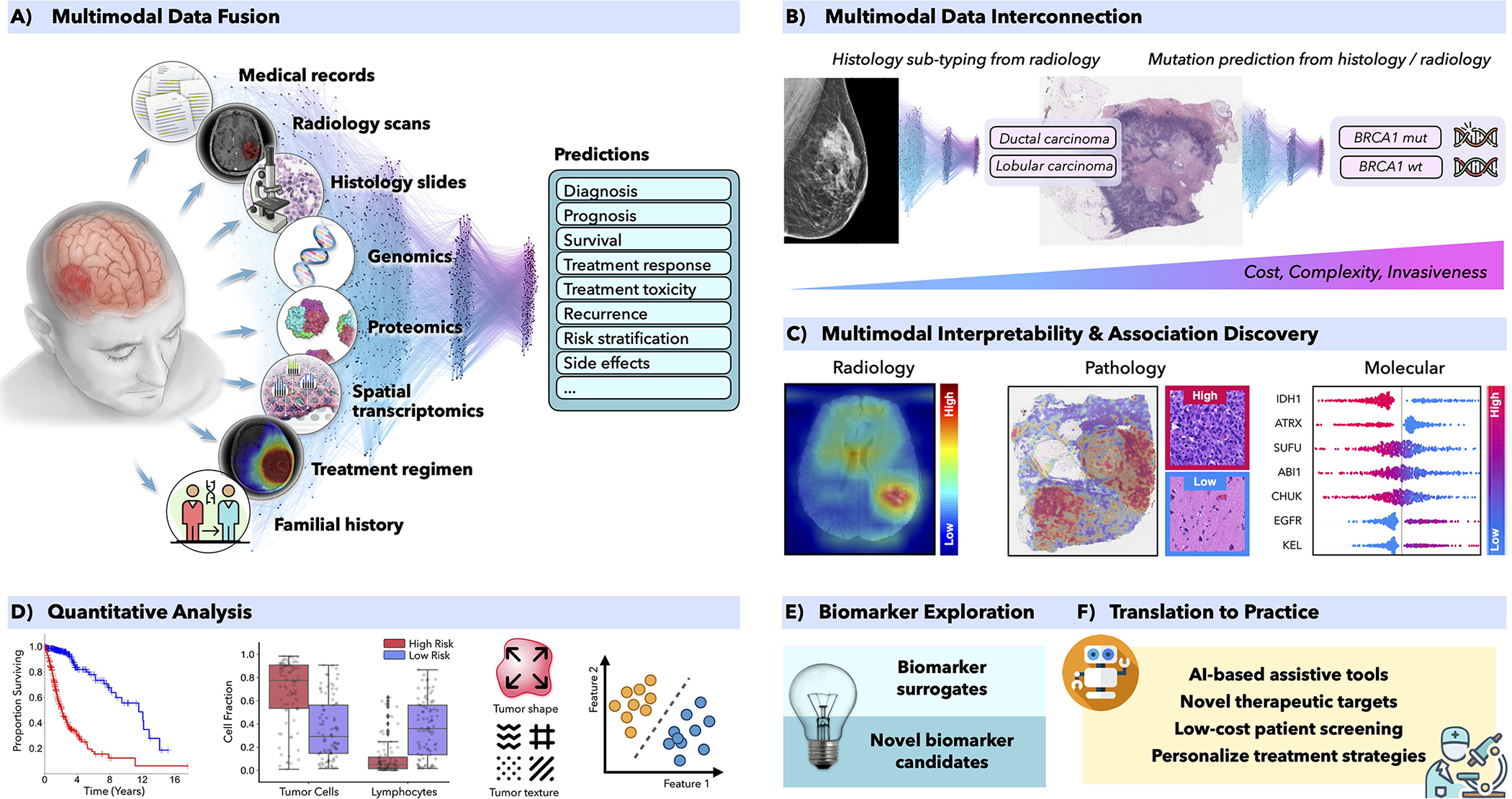
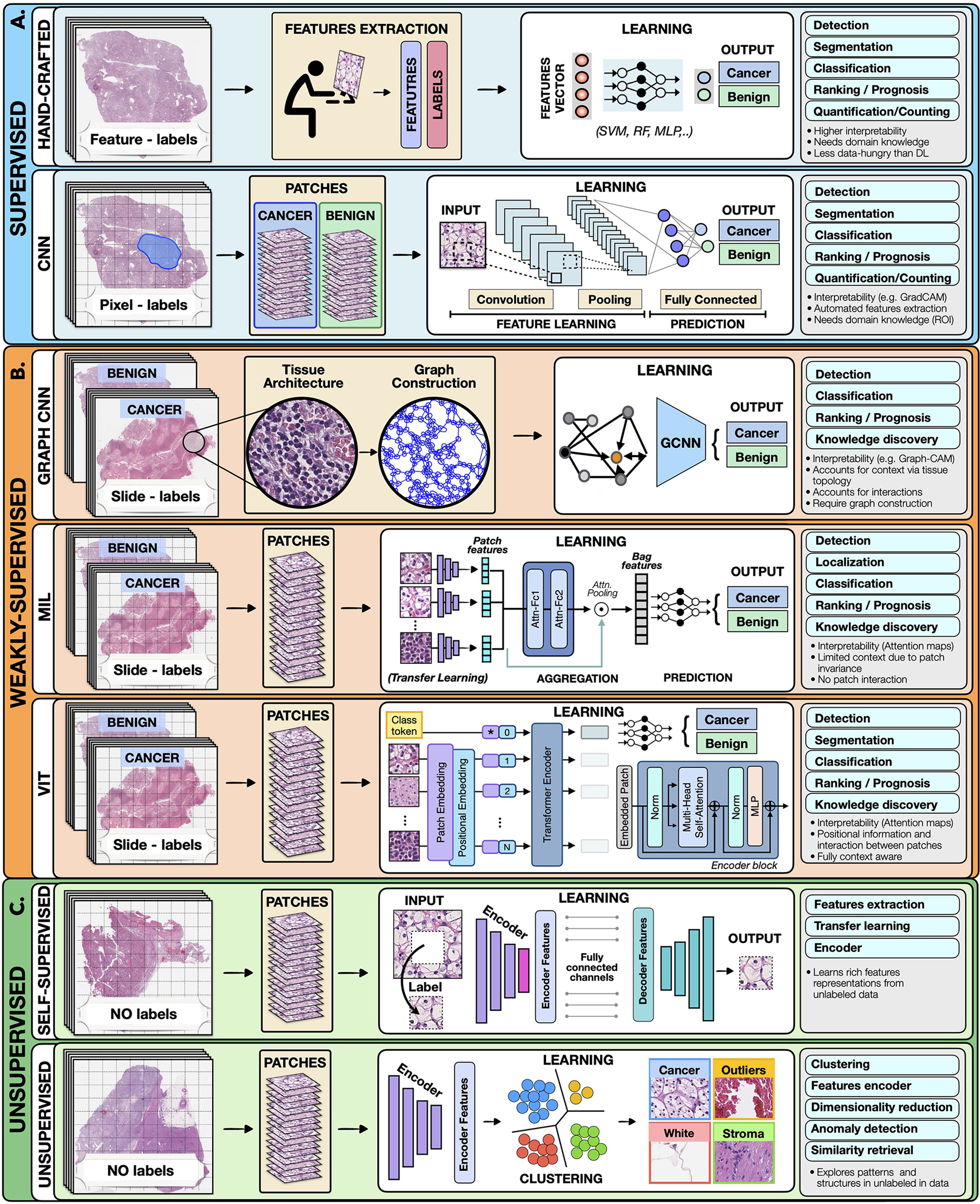
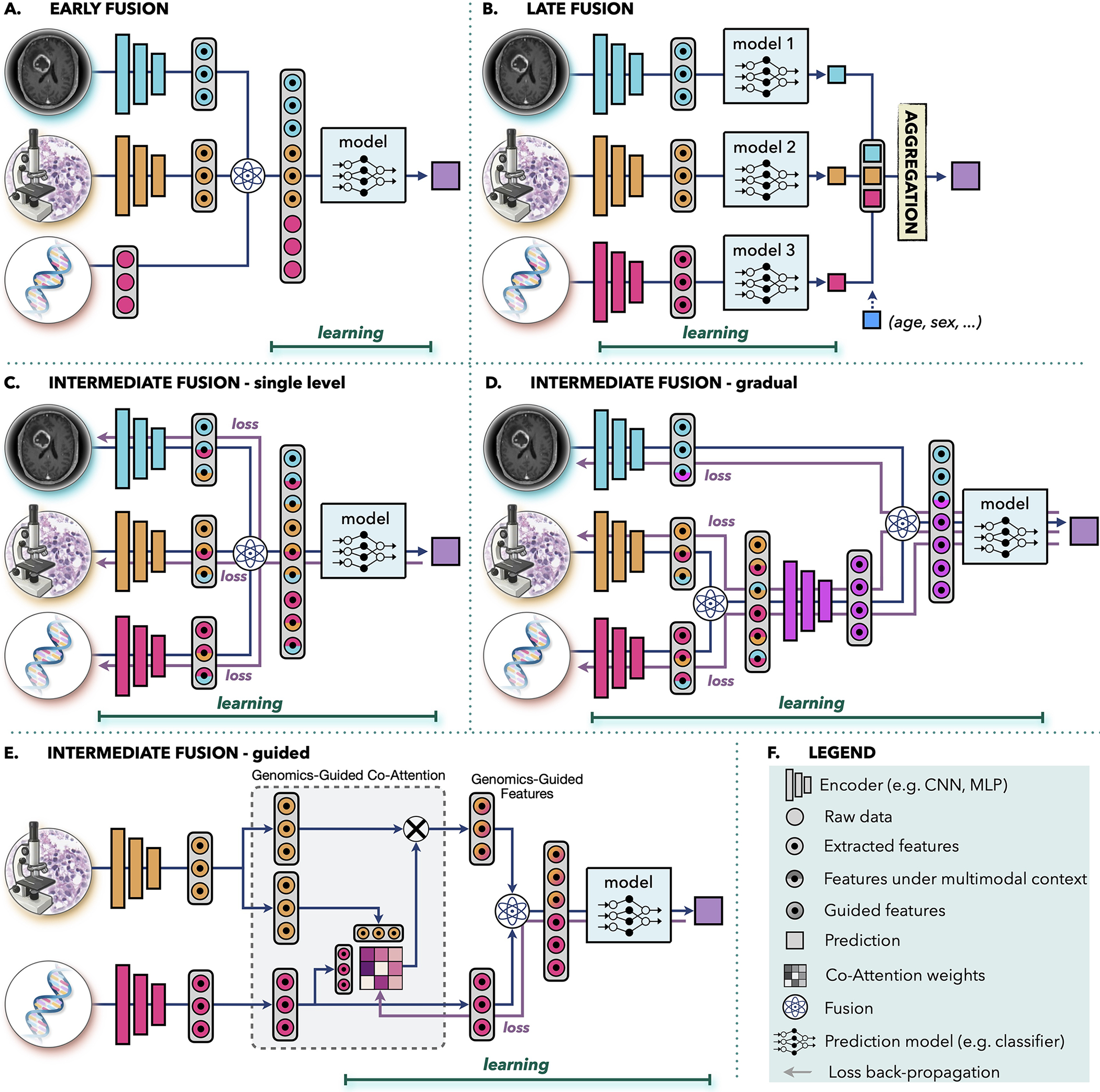
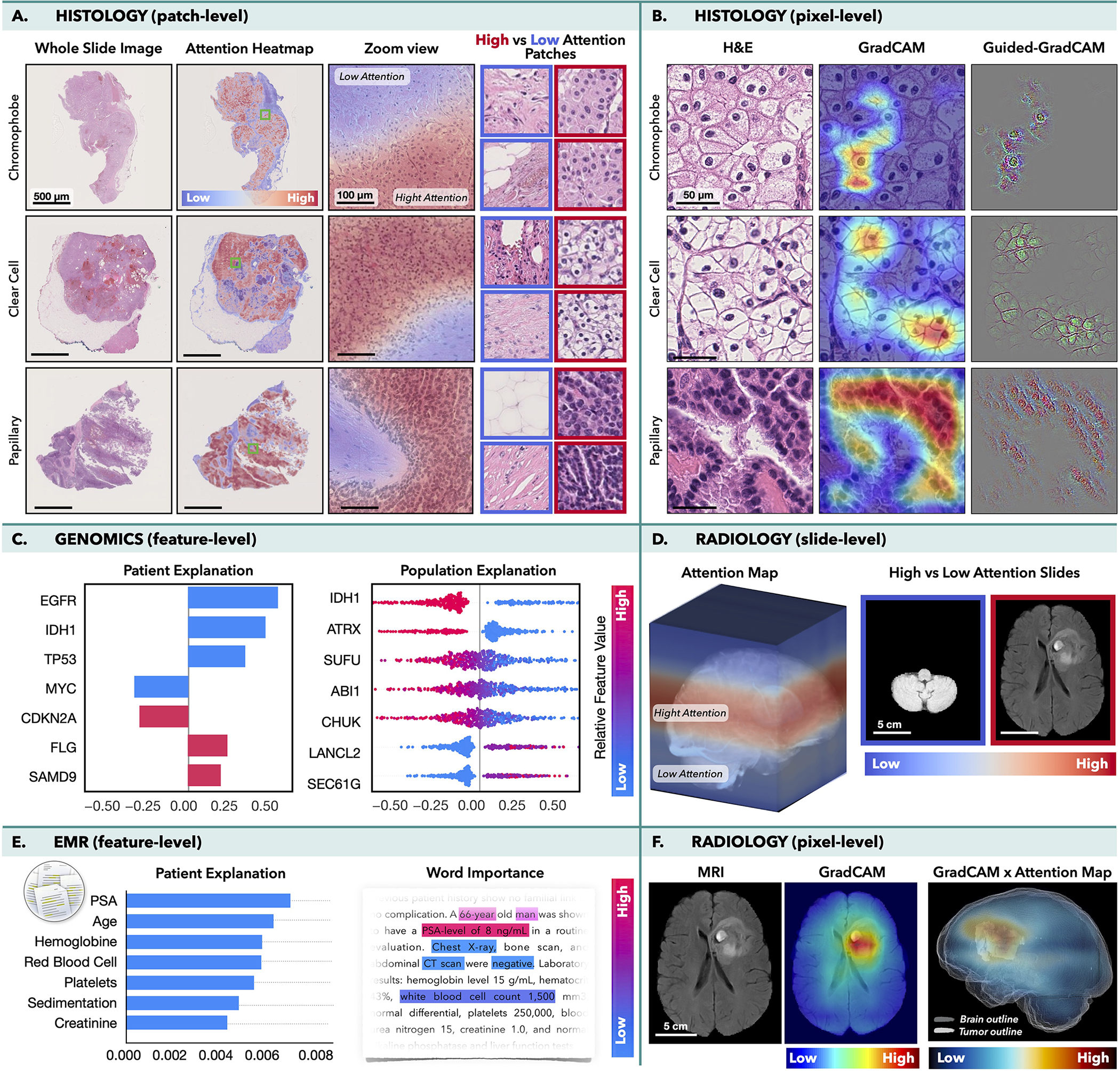
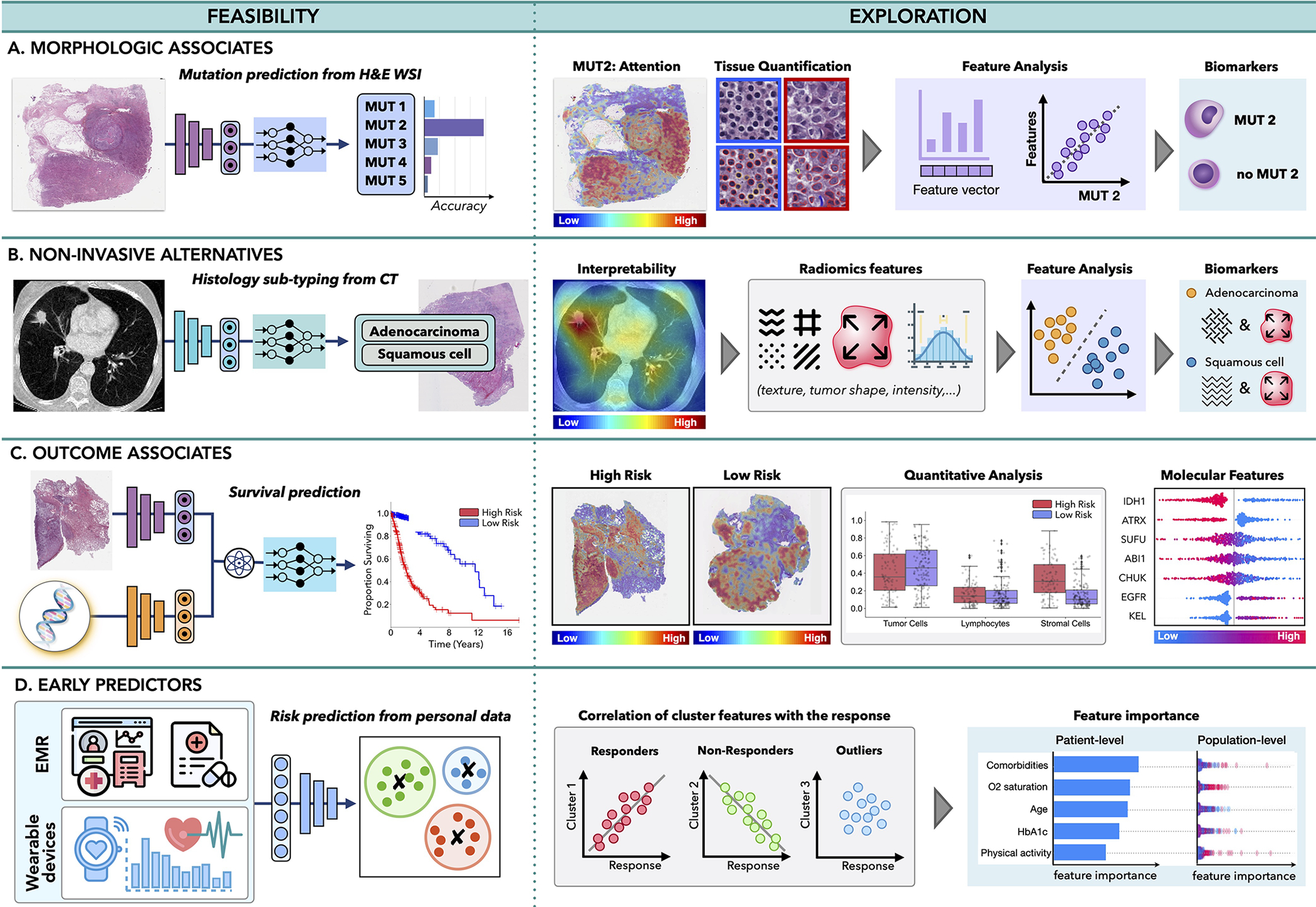
In oncology, the patient state is characterized by a whole spectrum of modalities, ranging from radiology, histology, and genomics to electronic health records. Current artificial intelligence (AI) models operate mainly in the realm of a single modality, neglecting the broader clinical context, which inevitably diminishes their potential. Integration of different data modalities provides opportunities to increase robustness and accuracy of diagnostic and prognostic models, bringing AI closer to clinical practice. AI models are also capable of discovering novel patterns within and across modalities suitable for explaining differences in patient outcomes or treatment resistance. The insights gleaned from such models can guide exploration studies and contribute to the discovery of novel biomarkers and therapeutic targets. To support these advances, here we present a synopsis of AI methods and strategies for multimodal data fusion and association discovery. We outline approaches for AI interpretability and directions for AI-driven exploration through multimodal data interconnections. We examine challenges in clinical adoption and discuss emerging solutions.
Keywords: AI in oncology; deep learning; deep learning in oncology; multimodal AI; multimodal fusion; multimodal integration.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests F.M. and R.J.C. are inventors on a patent related to multimodal learning.
Figures
References
-
- Adebayo J, Gilmer J, Muelly M, Goodfellow I, Hardt M, and Kim B. Sanity checks for saliency maps. In Bengio S, Wallach H, Larochelle H, Grauman K, Cesa-Bianchi N, and Garnett R, editors, Advances in Neural Information Processing Systems, volume 31. Curran Associates, Inc., 2018.
-
- Ahmedt-Aristizabal D, Armin MA, Denman S, Fookes C, and Petersson L. A survey on graph-based deep learning for computational histopathology. Computerized Medical Imaging and Graphics, page 102027, 2021. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
