

Alcohol Intake as a Risk Factor for Acute Stroke: The INTERSTROKE Study
- PMID: 36220600
- PMCID: PMC9841450
- DOI: 10.1212/WNL.0000000000201388
Alcohol Intake as a Risk Factor for Acute Stroke: The INTERSTROKE Study
Abstract
Background and objectives: There is uncertainty about the association between alcohol consumption and stroke, particularly for low-moderate intake. We explored these associations in a large international study.
Methods: INTERSTROKE, a case-control study, is the largest international study of risk factors for acute stroke. Alcohol consumption was self-reported and categorized by drinks/week as low (1-7), moderate (7-14 for females and 7-21 for males), or high (>14 for females and >21 for males). Heavy episodic drinking (HED) was defined as >5 drinks on ≥1 day per month. Multivariable conditional logistic regression was used to determine associations.
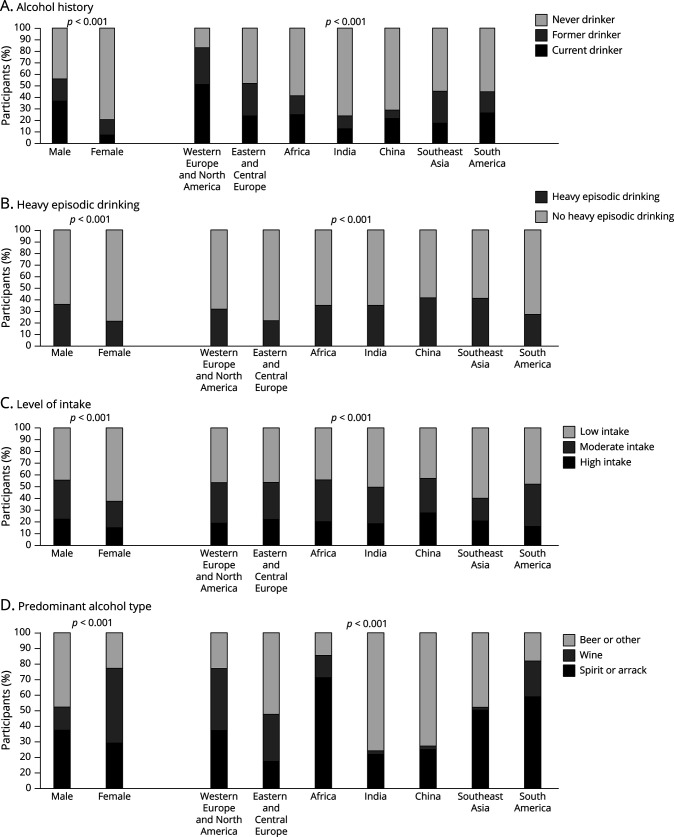
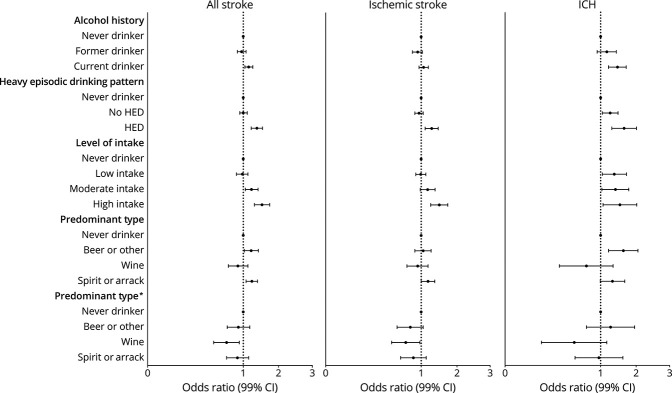
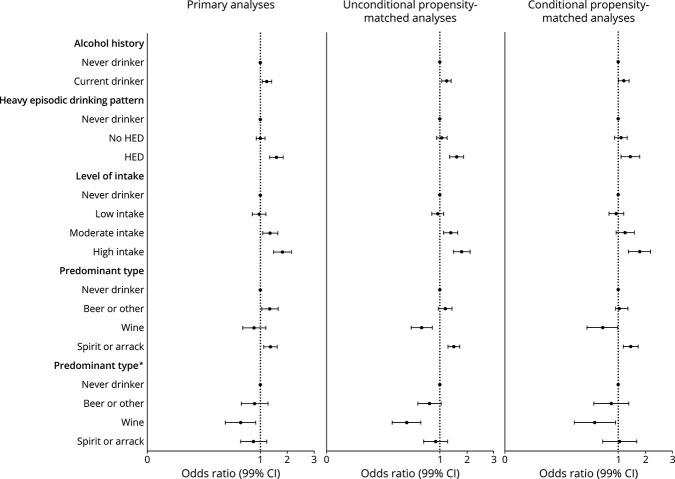
Results: We included 12,913 cases and 12,935 controls; 25.0% (n = 6,449) were current drinkers, 16.7% (n = 4,318) former drinkers, and 58.3% (n = 15,076) never drinkers. Current drinkers were younger, male, smokers, active, and with higher-paid occupations. Current drinking was associated with all stroke (OR 1.14; 95% CI 1.04-1.26) and intracerebral hemorrhage (ICH) (OR 1.50, 95% CI 1.21-1.84) but not ischemic stroke (OR 1.06; 95% CI 0.95-1.19). HED pattern was associated with all stroke (OR 1.39; 95% CI 1.21-1.59), ischemic stroke (OR 1.29; 95% CI 1.10-1.51), and ICH (OR 1.76; 95% CI 1.31-2.36). High level of alcohol intake was consistently associated with all stroke, ischemic stroke, and ICH. Moderate intake was associated with all stroke and ICH but not ischemic stroke. Low alcohol intake was not associated with stroke overall, but there were regional differences; low intake was associated with reduced odds of stroke in Western Europe/North America (OR 0.66; 95% CI 0.45-0.96) and increased odds in India (OR 2.18; 95% CI 1.42-3.36) (p-interaction 0.037). Wine consumption was associated with reduced odds of all stroke and ischemic stroke but not ICH. The magnitudes of association were greatest in those without hypertension and current smokers.
Discussion: High and moderate intake were associated with increased odds of stroke, whereas low intake was not associated with stroke. However, there were important regional variations, which may relate to differences in population characteristics of alcohol consumers, types or patterns of consumption.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Feigin VL, Forouzanfar MH, Krishnamurthi R, et al. ; Global Burden of Diseases, Injuries, and Risk Factors Study 2010 GBD 2010 and the GBD Stroke Experts Group. Global and regional burden of stroke during 1990-2010: findings from the global burden of disease study 2010. Lancet. 2014;383(9913):245-254. - PMC - PubMed
-
- Johnston SC, Mendis S, Mathers CD. Global variation in stroke burden and mortality: estimates from monitoring, surveillance, and modelling. Lancet Neurol. 2009;8(4):345-354. - PubMed
-
- Lopez AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002-2030. Ann Trop Med Parasitol. 2006;100(5-6):481-499. - PubMed
-
- O'Donnell M, Yusuf S. Tackling the global burden of stroke: the need for large-scale international studies. Lancet Neurol. 2009;8(4):306-307. - PubMed
-
- Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet. 2009;373(9682):2223-2233. - PubMed