

Real-world study of overall survival with palbociclib plus aromatase inhibitor in HR+/HER2- metastatic breast cancer
- PMID: 36220852
- PMCID: PMC9553912
- DOI: 10.1038/s41523-022-00479-x
Real-world study of overall survival with palbociclib plus aromatase inhibitor in HR+/HER2- metastatic breast cancer
Abstract
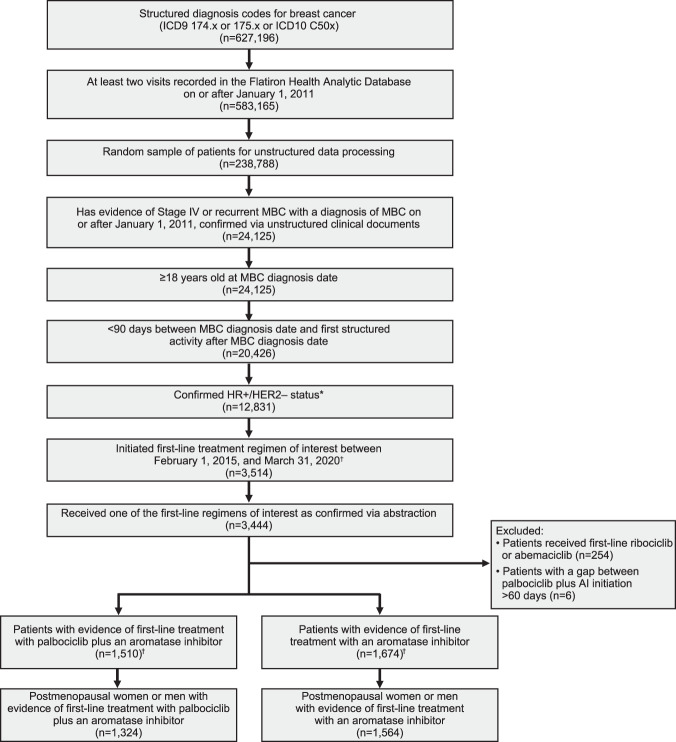
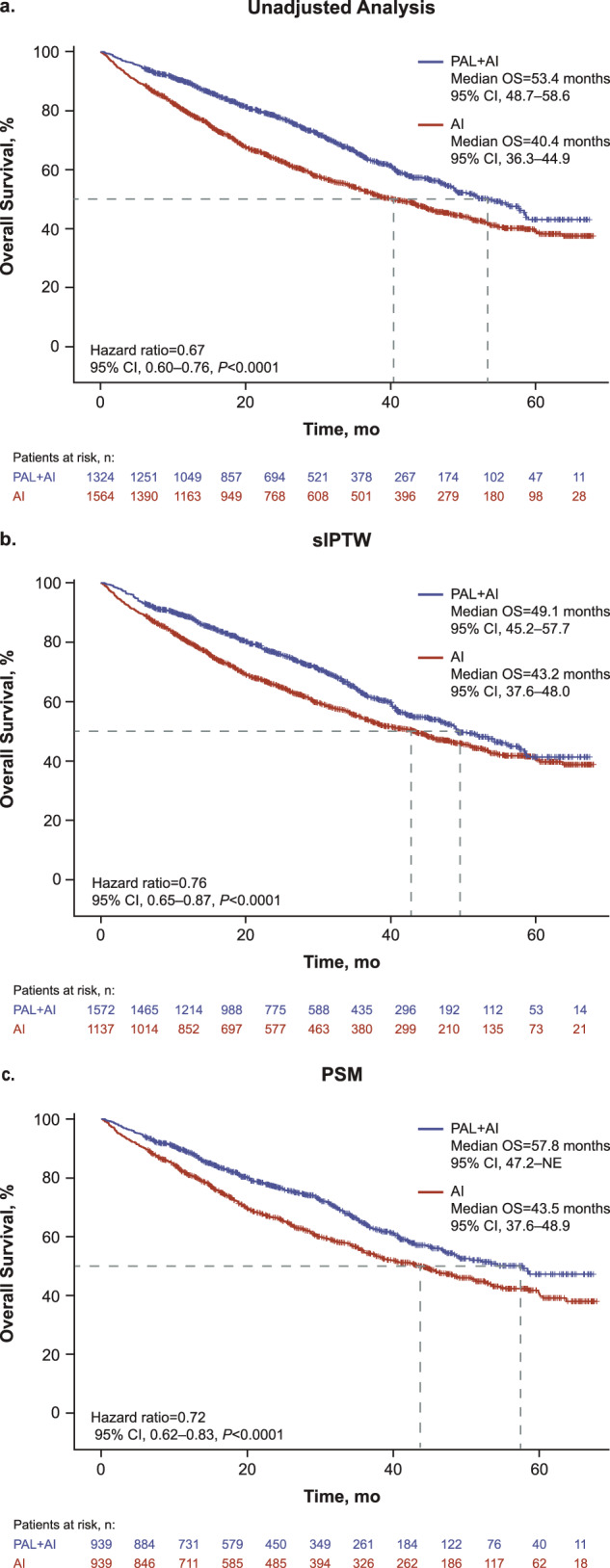
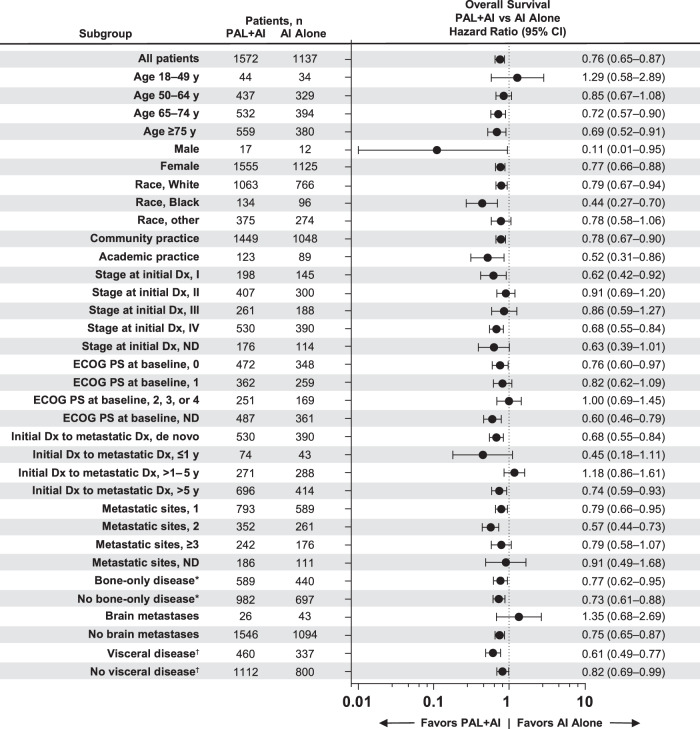
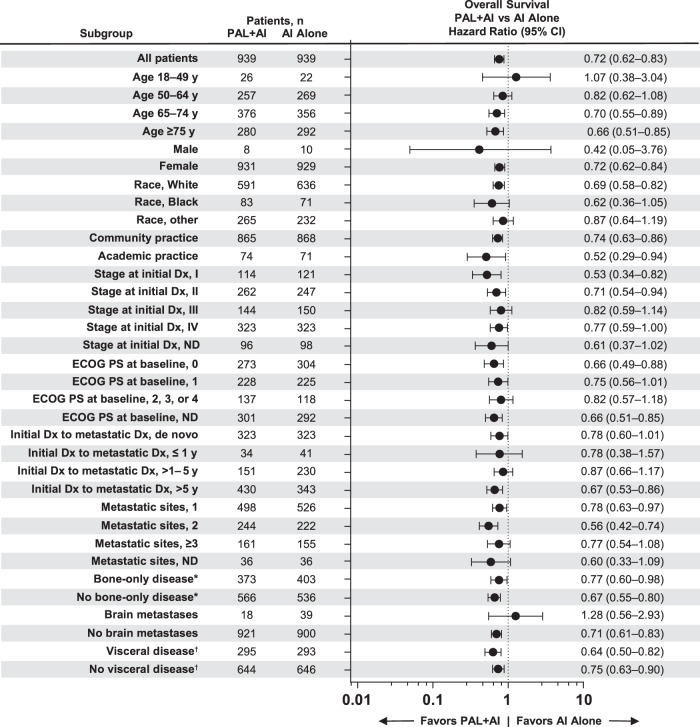
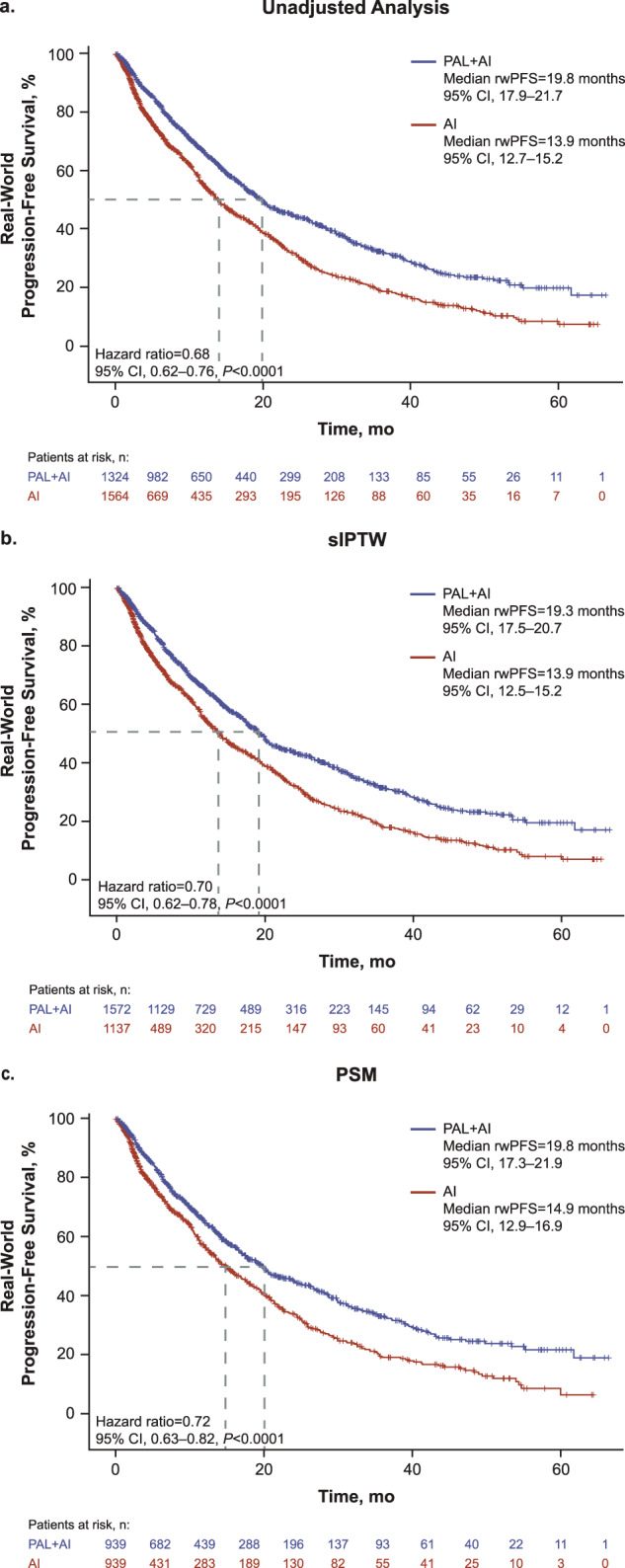
Data on real-world effectiveness of cyclin-dependent kinase 4/6 inhibitor combination therapy versus endocrine therapy alone are limited. The Flatiron Health Analytic Database was used to assess overall survival (OS) in patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2-) metastatic breast cancer (MBC) treated with first-line palbociclib plus an aromatase inhibitor (AI) versus an AI alone in routine US clinical practice. In total, 2888 patients initiated treatment during February 3, 2015-March 31, 2020, with a potential ≥6-month follow-up (cutoff date, September 30, 2020). After stabilized inverse probability treatment weighting, median OS (95% CI) is significantly longer among palbociclib versus AI recipients (49.1 [45.2-57.7] versus 43.2 [37.6-48.0] months; hazard ratio, 0.76 [95% CI, 0.65-0.87]; P < 0.0001). Progression-free survival (95% CI) is 19.3 (17.5-20.7) versus 13.9 (12.5-15.2) months, respectively (hazard ratio, 0.70 [95% CI, 0.62-0.78]; P < 0.0001). These data support first-line palbociclib plus an AI treatment for HR+/HER2- MBC.(Trial number NCT05361655).
© 2022. Pfizer Inc.
Conflict of interest statement
The authors declare no competing non-financial interests but the following competing financial interests: H.S.R. reports sponsored research to her institution from Pfizer Inc, Merck, Novartis, Eli Lilly, Roche, Daiichi-Sankyo, Seattle Genetics, Macrogenics, Sermonix, Boehringer Ingelheim, Polyphor, AstraZeneca, Ayala, and Gilead and honoraria from PUMA, Samsung, and Mylan. A.B. reports advisory/consultancy fees from Pfizer Inc. R.M.L. reports advisory/consultancy fees from Novartis, Eli Lilly, and Celcuity and research/grant funding from Pfizer Inc, Novartis, Eli Lilly, GlaxoSmithKline, Zentalis, Puma, and Celcuity. M.C. reports advisory/consultancy fees (Data Safety Monitoring Board or Advisory Board) from Merck and AstraZeneca; research grant/funding from Pfizer Inc, Menarini, Eli Lilly, and G1 Therapeutics; consulting fees from Novartis, Menarini, Eli Lilly, Sermonix, G1 Therapeutics, AstraZeneca, Pfizer Inc, and Foundation Medicine; and travel support from Foundation Medicine. M.A.T. reports research grant/funding from Pfizer Inc and Genentech, advisory/consulting fees from Centers for Disease Control and Oncohealth, and honoraria from MJH Life Sciences. G.C. reports consulting fees from Seagen, Roche, Novartis, Lilly, Daiichi Sankyo, Astra Zeneca, Pfizer, Sanofi, Pierre Fabre, and Gilead and fees for non-CME services (eg, speakers’ bureaus) from Lilly, Pfizer, and Daiichi Sankyo. R.S.F. reports consulting fees/honoraria from Pfizer Inc and research grant/funding from Pfizer Inc, Eli Lilly, and Novartis. A.D. reports research grant/funding from Pfizer Inc, Novartis, Calithera, and Genentech. X.L., B.L., L.M., and C.C. are employees of and stockholders in Pfizer Inc.
Figures
References
-
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: Female breast cancer subtypes. https://seer.cancer.gov/statfacts/html/breast-subtypes.html (2022). (Accessed October 2022).
-
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Breast Cancer V.3.2022. © National Comprehensive Cancer Network, Inc. 2022. All rights reserved. Accessed May 13, 2022. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419. (Accessed October 2022).
-
- IBRANCE® capsules (palbociclib). Full Prescribing Information, Pfizer Inc, New York, NY. https://labeling.pfizer.com/ShowLabeling.aspx?id=2191 (2019). (Accessed October 2022).
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
