

Improved Survival After Liver Transplantation for Patients With Human Immunodeficiency Virus (HIV) and HIV/Hepatitis C Virus Coinfection in the Integrase Strand Transfer Inhibitor and Direct-Acting Antiviral Eras
- PMID: 36221143
- PMCID: PMC10169442
- DOI: 10.1093/cid/ciac821
Improved Survival After Liver Transplantation for Patients With Human Immunodeficiency Virus (HIV) and HIV/Hepatitis C Virus Coinfection in the Integrase Strand Transfer Inhibitor and Direct-Acting Antiviral Eras
Abstract
Background: People with human immunodeficiency virus (HIV) with and without hepatitis C virus (HCV) coinfection had poor outcomes after liver transplant (LT). Integrase strand transfer inhibitors (INSTIs) and direct-acting antivirals (DAAs) have changed the treatment landscape for HIV and HCV, respectively, but their impact on LT outcomes remains unclear.
Methods: This retrospective analysis of adults with HIV monoinfection (n = 246) and HIV/HCV coinfection (n = 286) who received LT compared mortality in patients with HIV who received LT before versus after approval of INSTIs and in patients with HIV/HCV coinfection who received LT before versus after approval of DAAs. In secondary analysis, we compared the outcomes in the different eras with those of propensity score-matched control cohorts of LT recipients without HIV or HCV infection.
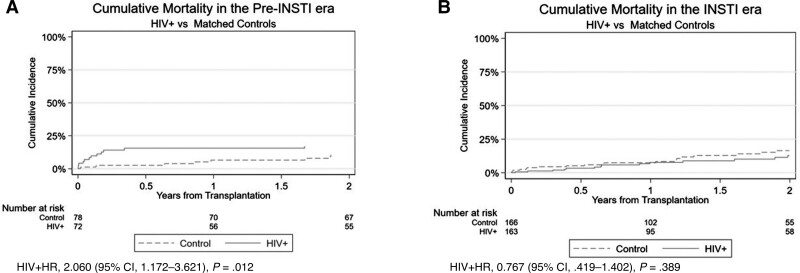
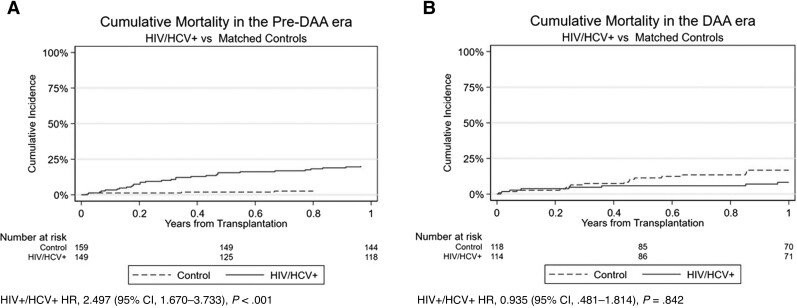
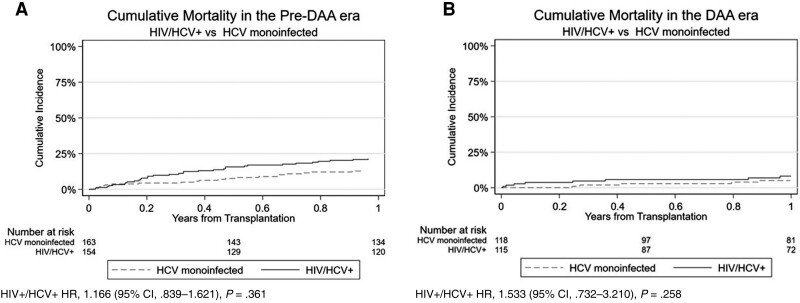
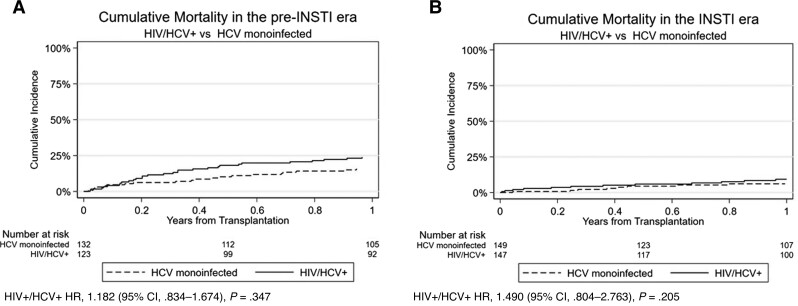
Results: LT recipients with HIV monoinfection did not experience a significant improvement in survival between the pre-INSTI and INSTI recipients with HIV (adjusted hazard ratio [aHR], 0.70 [95% confidence interval {CI}, .36-1.34]). However, recipients with HIV/HCV coinfection in the DAA era had a 47% reduction (aHR, 0.53 [95% CI, .31-9.2] in 1-year mortality compared with coinfected recipients in the pre-DAA era. Compared to recipients without HIV or HCV, HIV-monoinfected recipients had higher mortality during the pre-INSTI era, but survival was comparable between groups during the INSTI era. HIV/HCV-coinfected recipients also experienced comparable survival during the DAA era compared to recipients without HCV or HIV.
Conclusions: Post-LT survival for people with HIV monoinfection and HIV/HCV coinfection has improved with the introduction of INSTI and DAA therapy, suggesting that LT has become safer in these populations.
Keywords: DAA; HCV; HIV; INSTI; transplant.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Figures
References
-
- Gridelli B, Remuzzi G. Strategies for making more organs available for transplantation. N Engl J Med 2000; 343:404–10. - PubMed
-
- Shingina A, Dewitt PE, Dodge JL, et al. . Future trends in demand for liver transplant: birth cohort effects among patients with NASH and HCC. Transplantation 2019; 103:140–8. - PubMed
-
- Cooper C, Kanters S, Klein M, et al. . Liver transplant outcomes in HIV-infected patients: a systematic review and meta-analysis with synthetic cohort. AIDS 2011; 25:777–86. - PubMed
-
- Miro JM, Montejo M, Castells L, et al. . Outcome of HCV/HIV-coinfected liver transplant recipients: a prospective and multicenter cohort study. Am J Transplant 2012; 12:1866–76. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
