

Sensitivity and specificity analyses of COVID-19 screening protocol for emergency medical services: A STARD-compliant population-based retrospective study
- PMID: 36221409
- PMCID: PMC9541059
- DOI: 10.1097/MD.0000000000030902
Sensitivity and specificity analyses of COVID-19 screening protocol for emergency medical services: A STARD-compliant population-based retrospective study
Abstract
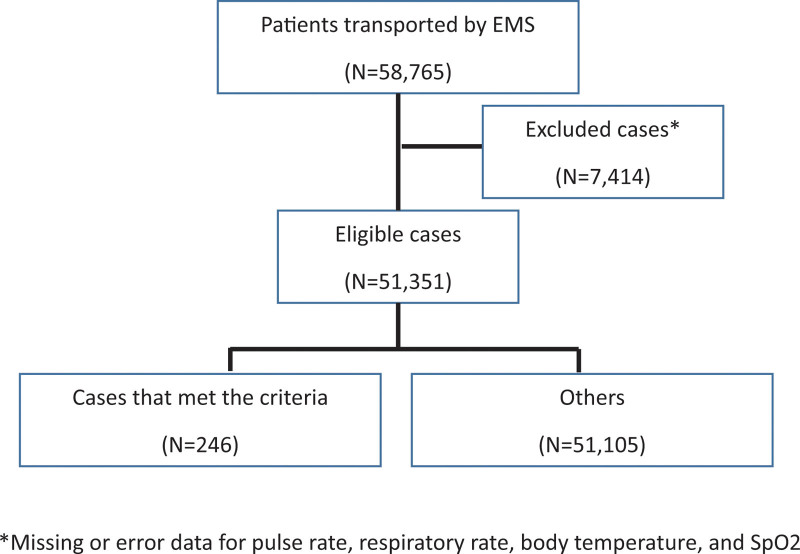
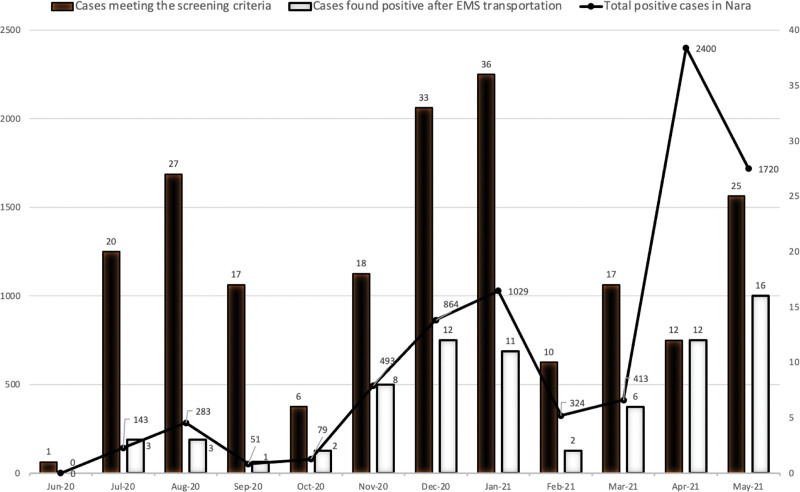
During the novel coronavirus disease (COVID-19) pandemic, emergency medical services (EMS) has borne a huge burden in transporting emergency patients. However, the protocol's effect on identifying emergency patients who are likely to have COVID-19 is unknown. We aimed to evaluate the diagnostic accuracy of a prehospital COVID-19 screening protocol for EMS. We conducted this population-based retrospective study in Nara Prefecture, Japan. The Nara Prefectural Government implemented a screening protocol for COVID-19 comprising the following symptom criteria (fever, cough, sore throat, headache, malaise, dysgeusia, or anosmia) and epidemiological criteria (contact history with confirmed COVID-19 cases or people with upper respiratory symptoms, or travel to areas with high infection rate). A patient meeting at least one criterion of each class was considered positive. We evaluated all 51,351 patients from the regional EMS database of the Nara Prefecture (emergency Medical Alliance for Total Coordination of Healthcare) who were registered from June 15, 2020 to May 31, 2021 and had results of COVID-19 reverse transcription polymerase chain reaction (RT-PCR) tests. We assessed the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of this protocol. We also assessed how these outcomes changed by adding vital signs and conducted a 10-fold and 100-fold prevalence simulation. The screening protocol was used for 246/51351 patients (0.5%). Among them, 31 tested positive after EMS transportation. This protocol's sensitivity, specificity, PPV, and NPV were 40.8%, 99.6%, 12.6%, and 99.9%, respectively. With the addition of ≥2 vital signs (body temperature ≥37.5 °C, respiratory rate ≥20 breaths/minute, and oxygen saturation <90%), sensitivity and PPV changed to 61.8% and 1.0%, respectively, while NPV remained 99.9%. With a 10-fold and 100-fold increase in disease, the protocol PPV would be 59.0% and 94.3%, and NPV would be 99.1% and 90.7%, respectively, and with additional vital signs, PPV would be 8.9% and 53.1%, and NPV would be 99.4% and 93.2%, respectively. This COVID-19 screening protocol helped enable EMS transport for patients with COVID-19 with a PPV of 12.6%. Adding other vital sign variables may improve its diagnostic value if the prevalence rate increases.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Detection of patients with COVID-19 by the emergency medical services in Lombardy through an operator-based interview and machine learning models.Emerg Med J. 2023 Nov 28;40(12):810-820. doi: 10.1136/emermed-2022-212853. Emerg Med J. 2023. PMID: 37775256 Free PMC article.
-
Should COVID-19 symptoms be used to cohort patients in the emergency department? A retrospective analysis.Am J Emerg Med. 2022 Apr;54:274-278. doi: 10.1016/j.ajem.2022.01.070. Epub 2022 Feb 6. Am J Emerg Med. 2022. PMID: 35220142 Free PMC article.
-
Virtualized clinical studies to assess the natural history and impact of gut microbiome modulation in non-hospitalized patients with mild to moderate COVID-19 a randomized, open-label, prospective study with a parallel group study evaluating the physiologic effects of KB109 on gut microbiota structure and function: a structured summary of a study protocol for a randomized controlled study.Trials. 2021 Apr 2;22(1):245. doi: 10.1186/s13063-021-05157-0. Trials. 2021. PMID: 33810796 Free PMC article.
-
Impact of the COVID-19 pandemic on prehospital emergency medical service: a scoping review.Front Public Health. 2025 Mar 19;13:1543150. doi: 10.3389/fpubh.2025.1543150. eCollection 2025. Front Public Health. 2025. PMID: 40177094 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
References
-
- World Health Organization. Coronavirus (COVID-19) dashboard. Available at: https://covid19.who.int/. Accessed August 16, 2022.
-
- He X, Lau EHY, Wu P, et al. . Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020;26:672–5. - PubMed
-
- Kundel HL, Polansky M. Measurement of observer agreement. Radiology. 2003;228:303–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
