

Long-term outcomes following catheter ablation versus medical therapy in patients with persistent atrial fibrillation and heart failure with reduced ejection fraction
- PMID: 36221809
- PMCID: PMC11497222
- DOI: 10.1002/ejhf.2714
Long-term outcomes following catheter ablation versus medical therapy in patients with persistent atrial fibrillation and heart failure with reduced ejection fraction
Abstract
Aims: The ARC-HF and CAMTAF trials randomized patients with persistent atrial fibrillation (AF) and heart failure (HF) to early routine catheter ablation (ER-CA) versus pharmacological rate control (RC). After trial completion, delayed selective catheter ablation (DS-CA) was performed where clinically indicated in the RC group. We hypothesized that ER-CA would result in a lower risk of cardiovascular hospitalization and death versus DS-CA in this population.
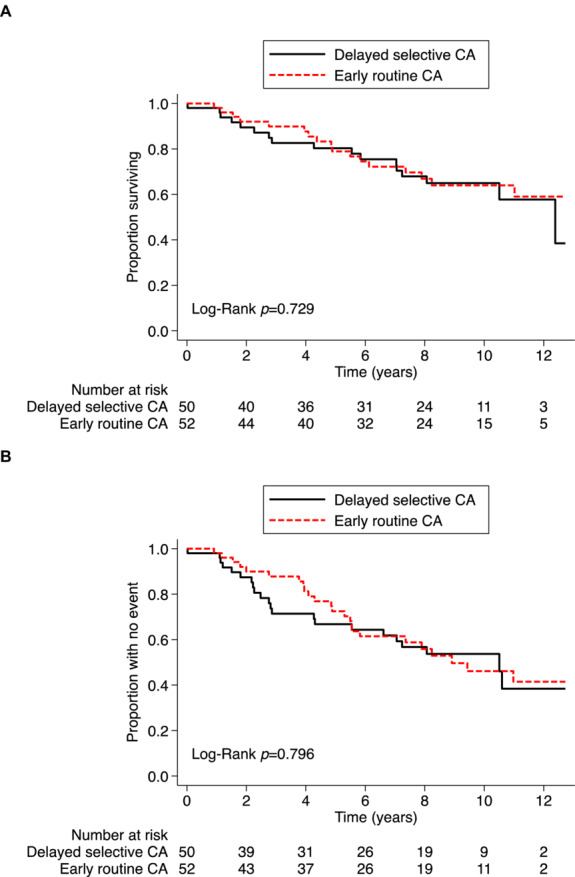
Methods and results: Overall, 102 patients were randomized (age 60 ± 11 years, left ventricular ejection fraction [LVEF] 31 ± 11%): 52 to ER-CA and 50 to RC. After 12 months, patients undergoing ER-CA had improved self-reported symptom scores, lower New York Heart Association class (i.e. better functional capacity), and higher LVEF compared to patients receiving RC alone. During a median follow-up of 7.8 (interquartile range 3.9-9.9) years, 27 (54%) patients in the RC group underwent DS-CA and 34 (33.3%) patients died, including 17 (32.7%) randomized to ER-CA and 17 (34.0%) randomized to RC. Compared with DS-CA, a strategy of ER-CA exhibited similar risk of all-cause mortality (adjusted hazard ratio [aHR] 0.89, 95% confidence interval [CI] 0.44-1.77, p = 0.731) and combined all-cause mortality or cardiovascular hospitalization (aHR 0.80, 95% CI 0.43-1.47, p = 0.467). However, analyses according to treatment received suggested an association between CA and improved outcomes versus RC (all-cause mortality: aHR 0.43, 95% CI 0.20-0.91, p = 0.028; all-cause mortality/cardiovascular hospitalization: aHR 0.48, 95% CI 0.24-0.94, p = 0.031).
Conclusions: In patients with persistent AF and HF, ER-CA produces similar long-term outcomes to a DS-CA strategy. The association between CA as a treatment received and improved outcomes means there is still a lack of clarity regarding the role of early CA in selected patients. Randomized trials are needed to clarify this question.
Keywords: Atrial fibrillation; Catheter ablation; Heart failure.
© 2022 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures


References
-
- Ling LH, Kistler PM, Kalman JM, Schilling RJ, Hunter RJ. Comorbidity of atrial fibrillation and heart failure. Nat Rev Cardiol. 2016;13:131–47. - PubMed
-
- Jones DG, Haldar SK, Hussain W, Sharma R, Francis DP, Rahman‐Haley SL, et al. A randomized trial to assess catheter ablation versus rate control in the management of persistent atrial fibrillation in heart failure. J Am Coll Cardiol. 2013;61:1894–903. - PubMed
-
- Hunter RJ, Berriman TJ, Diab I, Kamdar R, Richmond L, Baker V, et al. A randomized controlled trial of catheter ablation versus medical treatment of atrial fibrillation in heart failure (the CAMTAF trial). Circ Arrhythm Electrophysiol. 2014;7:31–8. - PubMed
-
- Khan MN, Jais P, Cummings J, Di Biase L, Sanders P, Martin DO, et al.; PABA‐CHF Investigators . Pulmonary‐vein isolation for atrial fibrillation in patients with heart failure. N Engl J Med. 2008;359:1778–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
