

Review
doi: 10.1259/bjr.20220121.
Epub 2022 Nov 25.
An update on uterine artery embolization for uterine leiomyomata and adenomyosis of the uterus
Affiliations
- PMID: 36222200
- PMCID: PMC9975358
- DOI: 10.1259/bjr.20220121
Item in Clipboard
Review
An update on uterine artery embolization for uterine leiomyomata and adenomyosis of the uterus
Br J Radiol.
2023 Mar.
Abstract
Uterine artery embolization (UAE) is an established technique to treat benign diseases of the uterus such as uterine leiomyomata (fibroids) and adenomyosis. This article reviews the use of UAE in these conditions and summarizes the evidence regarding safety and efficacy of the technique based on the current literature.
Figures

Digital subtraction angiography after selective catherization on the right ovarian artery. The typical downward course of the ovarian artery is depicted with its characteristic corkscrew appearance in its distal segment. The ovarian artery connects to the plexus vessels supplying a uterine leiomyoma (arrow).
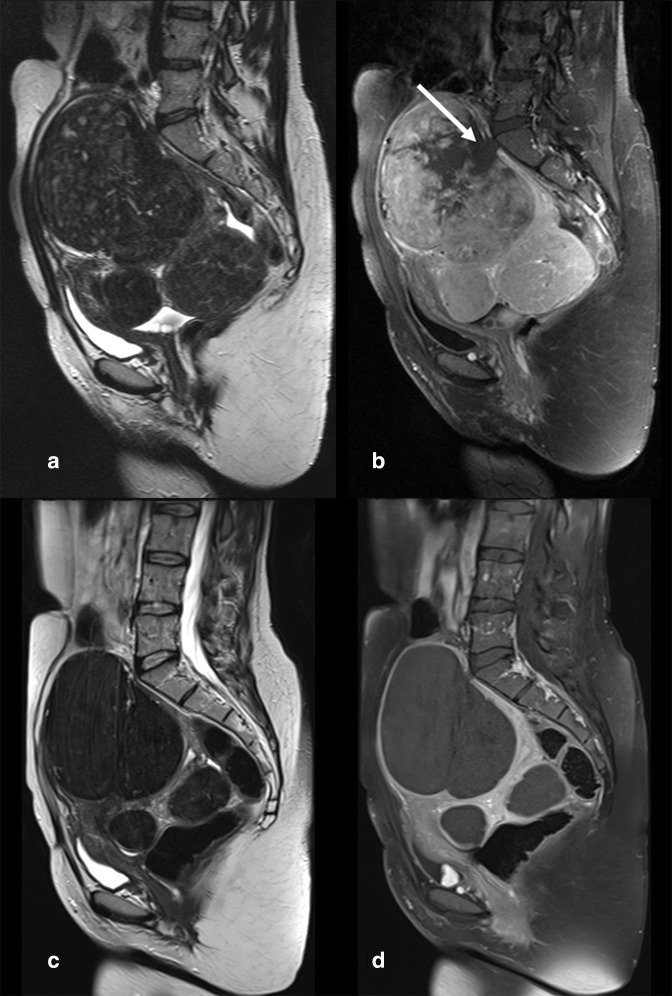
(a-d) T2w and T1w MR images before and after UAE. Multiple well-demarcated hypointense leiomyomata are depicted in (a). T1w contrast-enhanced imaging shows these fibroids are well-perfused except for a hypoperfused area next to the L5/S1 vertebra (white Arrow). A finding that sometimes can be seen in large polyfibroid uteri (B). T2w imaging obtained 6 months after UAE shows that the fibroids have undergone transformation due to infarction and now exhibit a homogenously hypointense signal intensity and moderate reduction in size (C). Contrast-enhanced T1w imaging confirms complete infraction of treated fibroids.
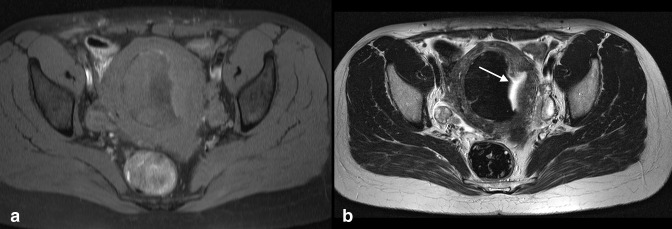
(a,b) T1w and T2w MR images 12 months after UAE. On T1w imaging an intramual/submucosal fibroid with a sharp hypointense, presumably calcified right-sided border is seen. The left sided part shows a broad stripe of hypointense tissue with an irregular hyperintense border(A). On T2w imaging the typical homogenous hypointense signal of the infarcted fibroid is bordered by hyperintense tissue in connection to the uterine cavity (arrow in B). This finding represents an area of sloughing and endometrial overgrowth. The patient reported a non-oderous discharge which was treated conservatively until resumption.
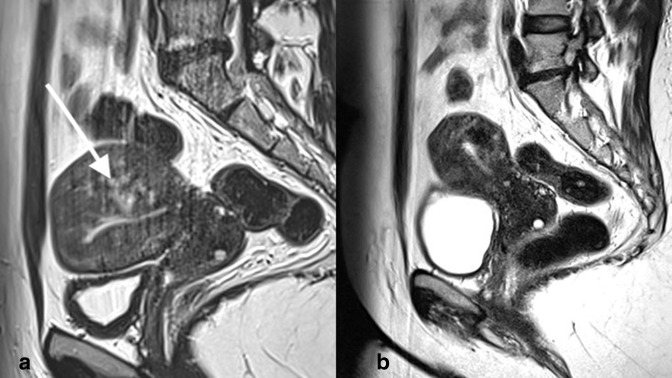
(a, b) T1w MR images before (a) and 12 months after (b) UAE for symptomatic adenomyosis. The uterus is asymmetrically enlarged. The junctional zone of the posterior wall is thickened and hyperintense spots as wells as claw-like protrusion extend from the endometrium into the myometrium (arrow in A). MR imaging 12 months later shows reduction in size of the uterus and the adenomyosis, with a hypointense area corresponding to infarcted adenomyotic tissue is seen in the posterior uterine wall. The patient reported a marked improvement regarding her bleeding symptoms (hypermenorrhea and dysmenorrhea).
References
-
- Geary RS, Gurol-Urganci I, Kiran A, Cromwell DA, Bansi-Matharu L, Shakespeare J, et al. Factors associated with receiving surgical treatment for menorrhagia in England and Wales: findings from a cohort study of the National heavy menstrual bleeding audit. BMJ Open 2019; 9(2): e024260. doi: 10.1136/bmjopen-2018-024260 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
