

The Dystonias
- PMID: 36222773
- PMCID: PMC10226676
- DOI: 10.1212/CON.0000000000001159
The Dystonias
Abstract
Purpose of review: This article discusses the most recent findings regarding the diagnosis, classification, and management of genetic and idiopathic dystonia.
Recent findings: A new approach to classifying dystonia has been created with the aim to increase the recognition and diagnosis of dystonia. Molecular biology and genetic studies have identified several genes and biological pathways involved in dystonia.
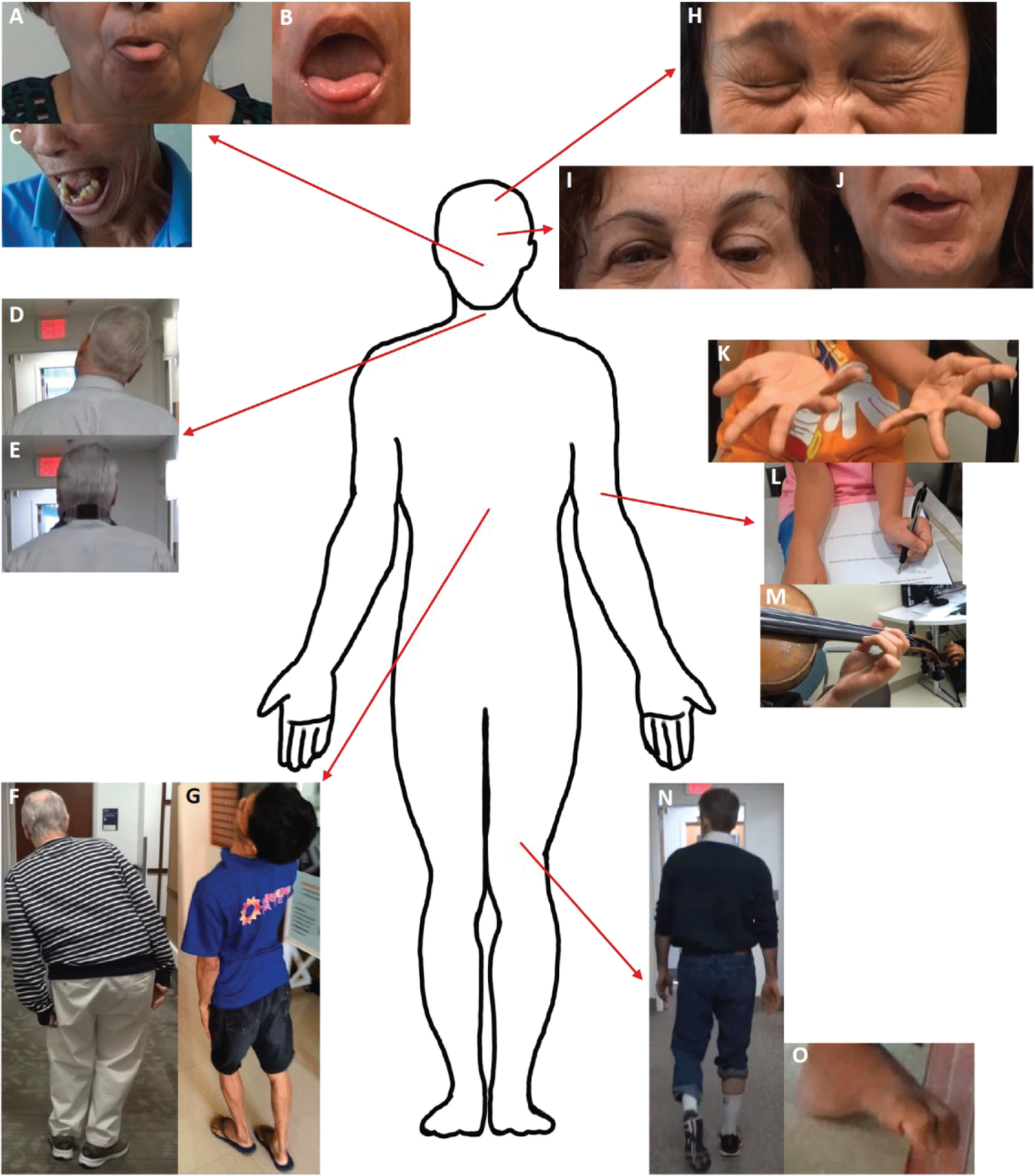
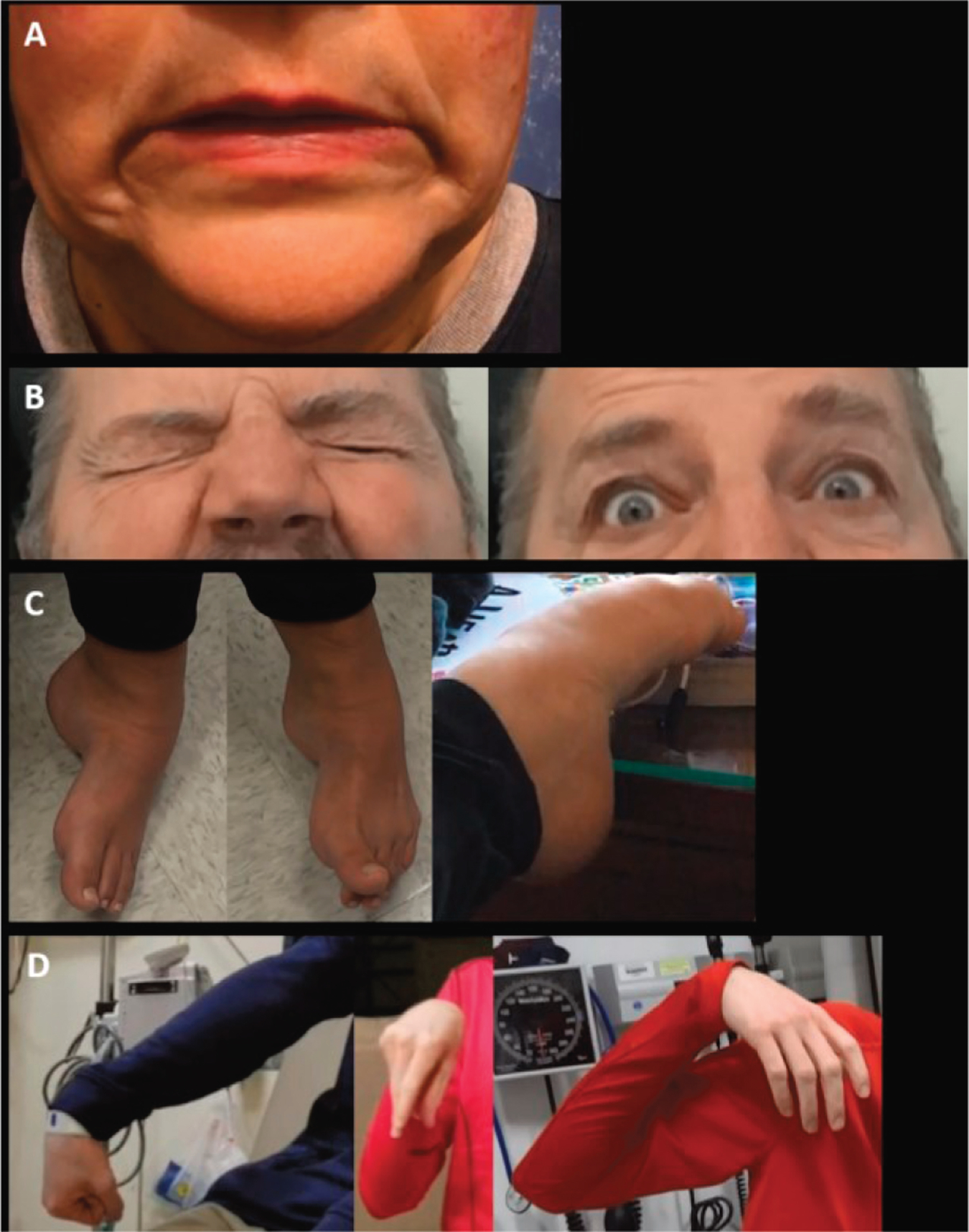
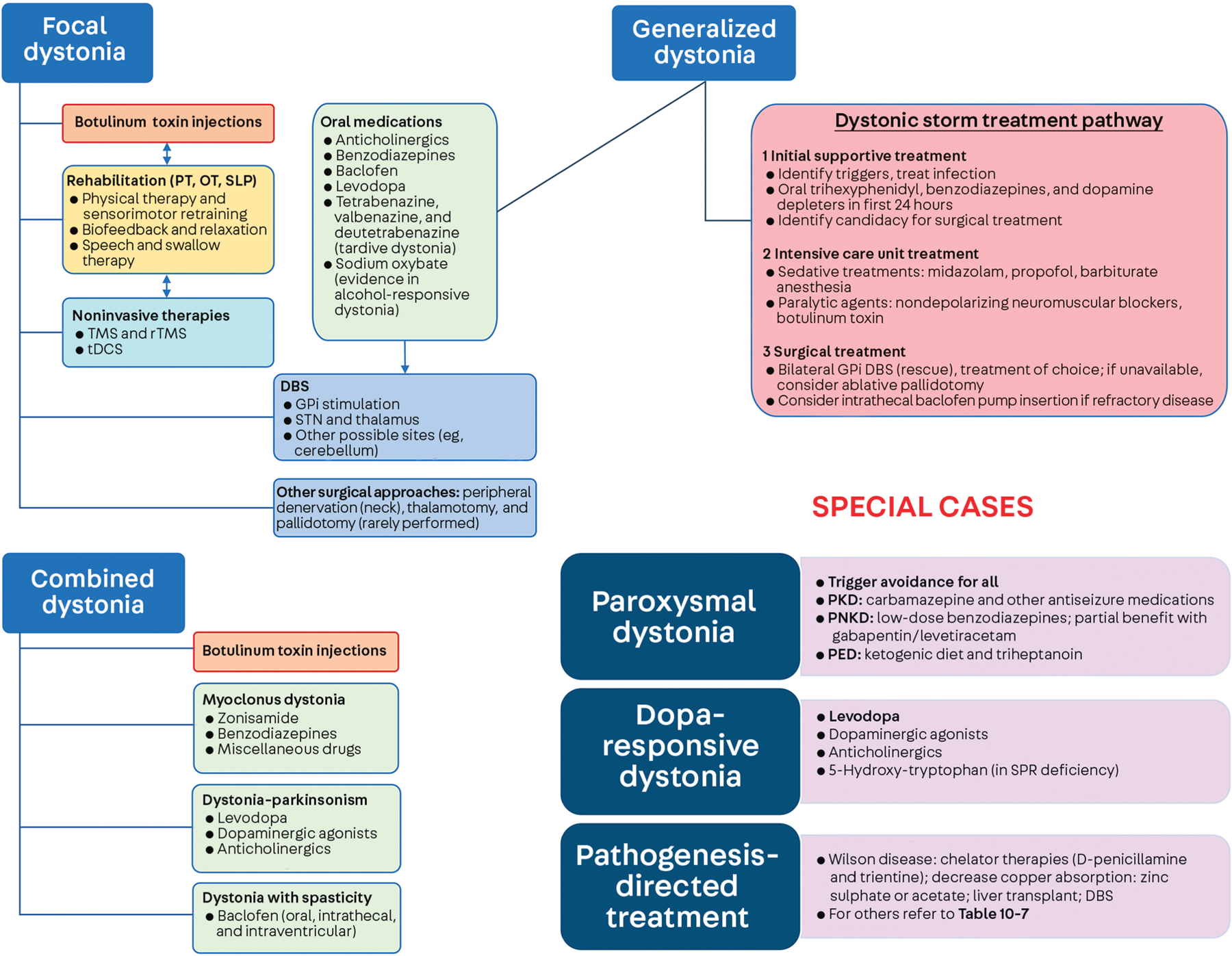
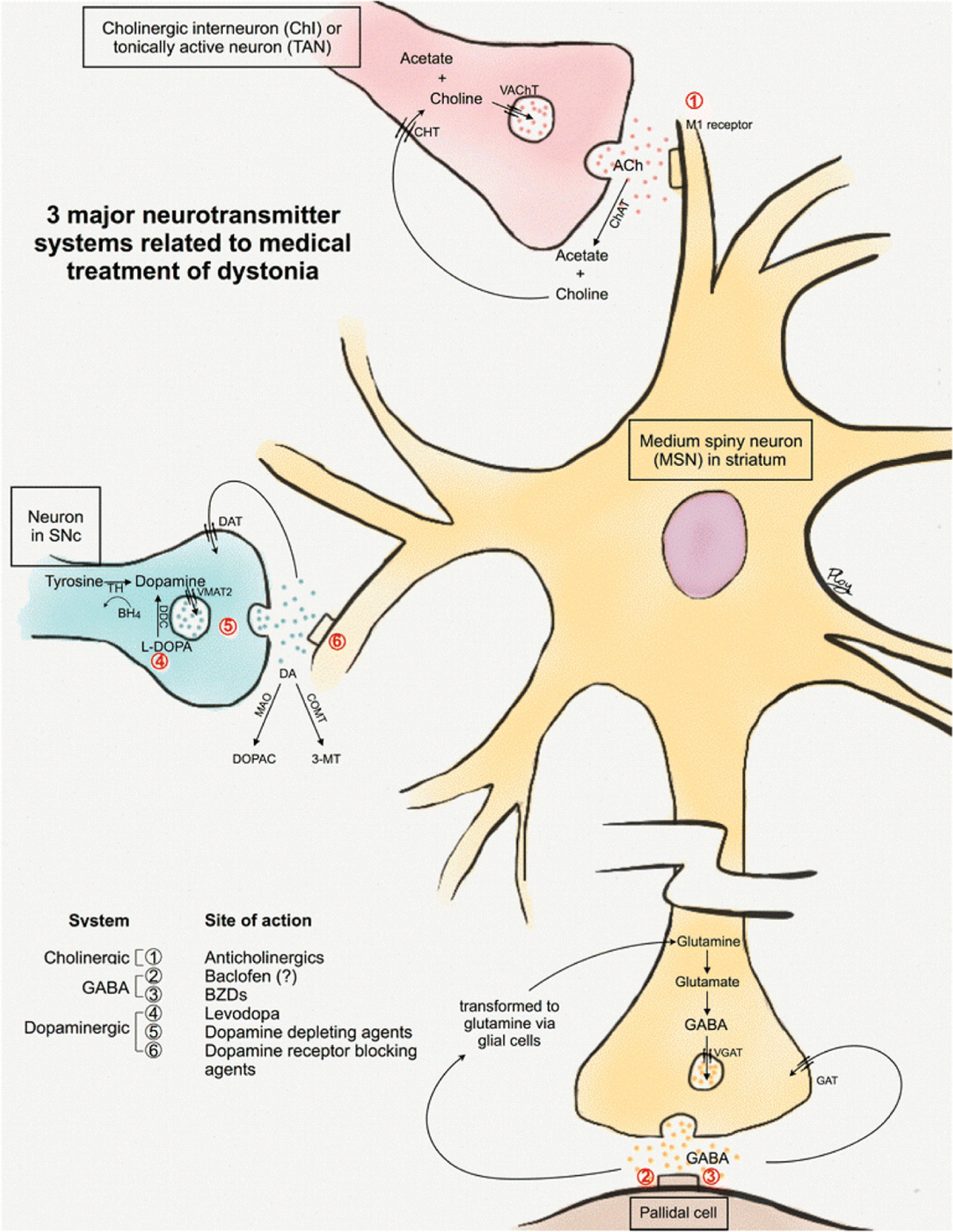
Summary: Dystonia is a common movement disorder involving abnormal, often twisting, postures and is a challenging condition to diagnose. The pathophysiology of dystonia involves abnormalities in brain motor networks in the context of genetic factors. Dystonia has genetic, idiopathic, and acquired forms, with a wide phenotypic spectrum, and is a common feature in complex neurologic disorders. Dystonia can be isolated or combined with another movement disorder and may be focal, segmental, multifocal, or generalized in distribution, with some forms only occurring during the performance of specific tasks (task-specific dystonia). Dystonia is classified by clinical characteristics and presumed etiology. The management of dystonia involves accurate diagnosis, followed by treatment with botulinum toxin injections, oral medications, and surgical therapies (mainly deep brain stimulation), as well as pathogenesis-directed treatments, including the prospect of disease-modifying or gene therapies.
Copyright © 2022 American Academy of Neurology.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials