

The Triage Capability of Laypersons: Retrospective Exploratory Analysis
- PMID: 36222793
- PMCID: PMC9607917
- DOI: 10.2196/38977
The Triage Capability of Laypersons: Retrospective Exploratory Analysis
Abstract
Background: Although medical decision-making may be thought of as a task involving health professionals, many decisions, including critical health-related decisions are made by laypersons alone. Specifically, as the first step to most care episodes, it is the patient who determines whether and where to seek health care (triage). Overcautious self-assessments (ie, overtriaging) may lead to overutilization of health care facilities and overcrowded emergency departments, whereas imprudent decisions (ie, undertriaging) constitute a risk to the patient's health. Recently, patient-facing decision support systems, commonly known as symptom checkers, have been developed to assist laypersons in these decisions.
Objective: The purpose of this study is to identify factors influencing laypersons' ability to self-triage and their risk averseness in self-triage decisions.
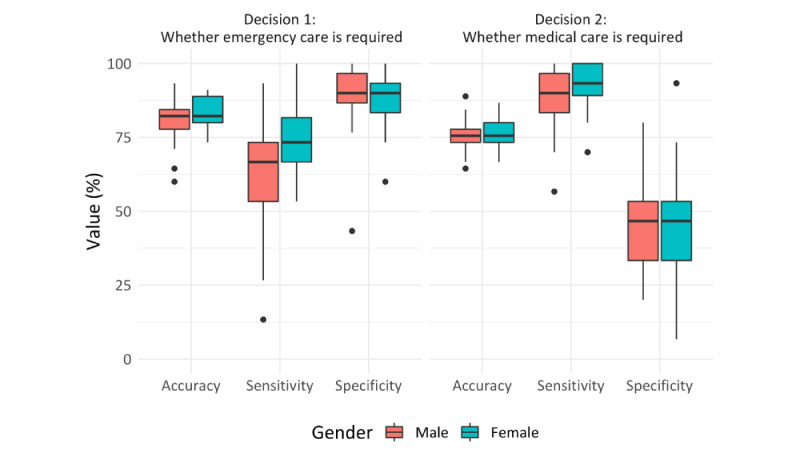
Methods: We analyzed publicly available data on 91 laypersons appraising 45 short fictitious patient descriptions (case vignettes; N=4095 appraisals). Using signal detection theory and descriptive and inferential statistics, we explored whether the type of medical decision laypersons face, their confidence in their decision, and sociodemographic factors influence their triage accuracy and the type of errors they make. We distinguished between 2 decisions: whether emergency care was required (decision 1) and whether self-care was sufficient (decision 2).
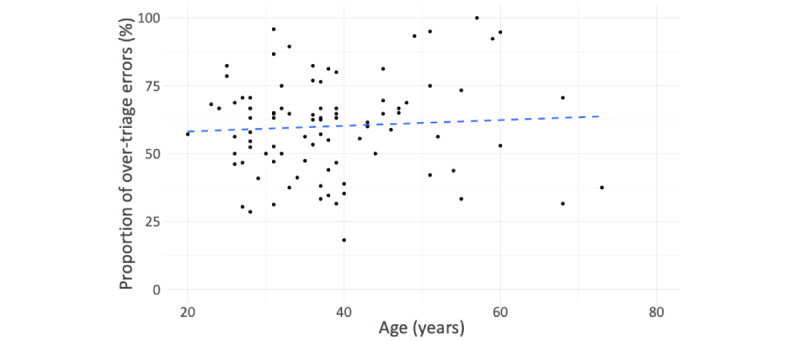
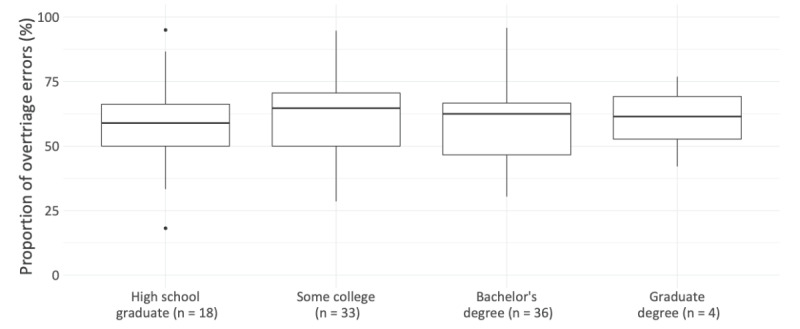
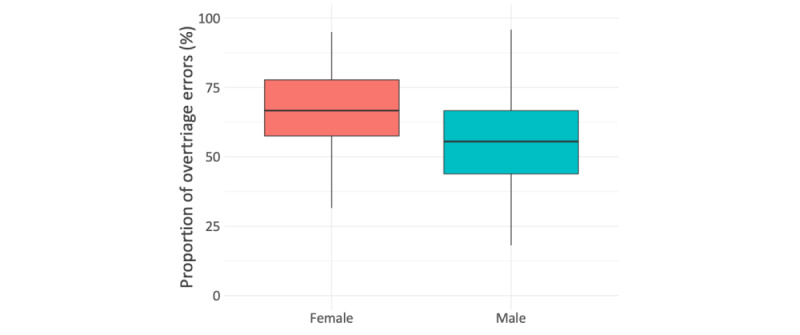
Results: The accuracy of detecting emergencies (decision 1) was higher (mean 82.2%, SD 5.9%) than that of deciding whether any type of medical care is required (decision 2, mean 75.9%, SD 5.25%; t>90=8.4; P<.001; Cohen d=0.9). Sensitivity for decision 1 was lower (mean 67.5%, SD 16.4%) than its specificity (mean 89.6%, SD 8.6%) whereas sensitivity for decision 2 was higher (mean 90.5%, SD 8.3%) than its specificity (mean 46.7%, SD 15.95%). Female participants were more risk averse and overtriaged more often than male participants, but age and level of education showed no association with participants' risk averseness. Participants' triage accuracy was higher when they were certain about their appraisal (2114/3381, 62.5%) than when being uncertain (378/714, 52.9%). However, most errors occurred when participants were certain of their decision (1267/1603, 79%). Participants were more commonly certain of their overtriage errors (mean 80.9%, SD 23.8%) than their undertriage errors (mean 72.5%, SD 30.9%; t>89=3.7; P<.001; d=0.39).
Conclusions: Our study suggests that laypersons are overcautious in deciding whether they require medical care at all, but they miss identifying a considerable portion of emergencies. Our results further indicate that women are more risk averse than men in both types of decisions. Layperson participants made most triage errors when they were certain of their own appraisal. Thus, they might not follow or even seek advice (eg, from symptom checkers) in most instances where advice would be useful.
Keywords: accuracy; care; care navigation; decision; decision support; digital health; emergency; error; female; health professional; male; medical; patient; patient-centered care; self-assessment; self-triage; sensitivity; support; symptom checker; triage; urgency assessment.
©Marvin Kopka, Markus A Feufel, Felix Balzer, Malte L Schmieding. Originally published in JMIR Formative Research (https://formative.jmir.org), 12.10.2022.
Conflict of interest statement
Conflicts of Interest: FB reports grants from German Federal Ministry of Education and Research, grants from German Federal Ministry of Health, grants from Berlin Institute of Health, personal fees from Elsevier Publishing, grants from Hans Böckler Foundation, other from Robert Koch Institute, grants from Einstein Foundation, grants from Berlin University Alliance, personal fees from Medtronic, and personal fees from GE Healthcare outside the submitted work.
Figures
Similar articles
-
Triage Accuracy of Symptom Checker Apps: 5-Year Follow-up Evaluation.J Med Internet Res. 2022 May 10;24(5):e31810. doi: 10.2196/31810. J Med Internet Res. 2022. PMID: 35536633 Free PMC article.
-
Benchmarking Triage Capability of Symptom Checkers Against That of Medical Laypersons: Survey Study.J Med Internet Res. 2021 Mar 10;23(3):e24475. doi: 10.2196/24475. J Med Internet Res. 2021. PMID: 33688845 Free PMC article.
-
Determinants of Laypersons' Trust in Medical Decision Aids: Randomized Controlled Trial.JMIR Hum Factors. 2022 May 3;9(2):e35219. doi: 10.2196/35219. JMIR Hum Factors. 2022. PMID: 35503248 Free PMC article.
-
The diagnostic and triage accuracy of digital and online symptom checker tools: a systematic review.NPJ Digit Med. 2022 Aug 17;5(1):118. doi: 10.1038/s41746-022-00667-w. NPJ Digit Med. 2022. PMID: 35977992 Free PMC article. Review.
-
Clinical Decision Support Systems for Triage in the Emergency Department using Intelligent Systems: a Review.Artif Intell Med. 2020 Jan;102:101762. doi: 10.1016/j.artmed.2019.101762. Epub 2019 Nov 17. Artif Intell Med. 2020. PMID: 31980099 Review.
Cited by
-
Protection Motivation Perspective Regarding the Use of COVID-19 Mobile Tracing Apps Among Public Users: Empirical Study.JMIR Form Res. 2023 Mar 1;7:e36608. doi: 10.2196/36608. JMIR Form Res. 2023. PMID: 36735838 Free PMC article.
-
Statistical refinement of patient-centered case vignettes for digital health research.Front Digit Health. 2024 Oct 21;6:1411924. doi: 10.3389/fdgth.2024.1411924. eCollection 2024. Front Digit Health. 2024. PMID: 39498100 Free PMC article.
-
The RepVig framework for designing use-case specific representative vignettes and evaluating triage accuracy of laypeople and symptom assessment applications.Sci Rep. 2024 Dec 23;14(1):30614. doi: 10.1038/s41598-024-83844-z. Sci Rep. 2024. PMID: 39715767 Free PMC article.
-
Characteristics of Users and Nonusers of Symptom Checkers in Germany: Cross-Sectional Survey Study.J Med Internet Res. 2023 Jun 20;25:e46231. doi: 10.2196/46231. J Med Internet Res. 2023. PMID: 37338970 Free PMC article.
-
Accuracy of online symptom assessment applications, large language models, and laypeople for self-triage decisions.NPJ Digit Med. 2025 Mar 25;8(1):178. doi: 10.1038/s41746-025-01566-6. NPJ Digit Med. 2025. PMID: 40133390 Free PMC article.
References
-
- Weissman JS, Rothschild JM, Bendavid E, Sprivulis P, Cook EF, Evans RS, Kaganova Y, Bender M, David-Kasdan J, Haug P, Lloyd J, Selbovitz LG, Murff HJ, Bates DW. Hospital workload and adverse events. Med Care. 2007 May;45(5):448–55. doi: 10.1097/01.mlr.0000257231.86368.09.00005650-200705000-00011 - DOI - PubMed
-
- Sun BC, Hsia RY, Weiss RE, Zingmond D, Liang L, Han W, McCreath H, Asch SM. Effect of emergency department crowding on outcomes of admitted patients. Ann Emerg Med. 2013 Jun;61(6):605–611.e6. doi: 10.1016/j.annemergmed.2012.10.026. https://europepmc.org/abstract/MED/23218508 S0196-0644(12)01699-X - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
