

Safety, Outcomes, and T-Cell Characteristics in Patients with Relapsed or Refractory MDS or CMML Treated with Atezolizumab in Combination with Guadecitabine
- PMID: 36222848
- PMCID: PMC9772102
- DOI: 10.1158/1078-0432.CCR-22-1810
Safety, Outcomes, and T-Cell Characteristics in Patients with Relapsed or Refractory MDS or CMML Treated with Atezolizumab in Combination with Guadecitabine
Abstract
Purpose: We hypothesized that resistance to hypomethylating agents (HMA) among patients with myelodysplastic syndrome (MDS) and chronic myelomonocytic leukemia (CMML) would be overcome by combining a programmed death-ligand 1 antibody with an HMA.
Patients and methods: We conducted a Phase I/II, multicenter clinical trial for patients with MDS not achieving an International Working Group response after at least 4 cycles of an HMA ("refractory") or progressing after a response ("relapsed") with 3+ or higher risk MDS by the revised International Prognostic Scoring System (IPSS-R) and CMML-1 or -2. Phase I consisted of a 3+3 dose-escalation design beginning with guadecitabine at 30 mg/m2 and escalating to 60 mg/m2 Days 1 to 5 with fixed-dose atezolizumab: 840 mg intravenously Days 8 and 22 of a 28-day cycle. Primary endpoints were safety and tolerability; secondary endpoints were overall response rate (ORR) and survival.
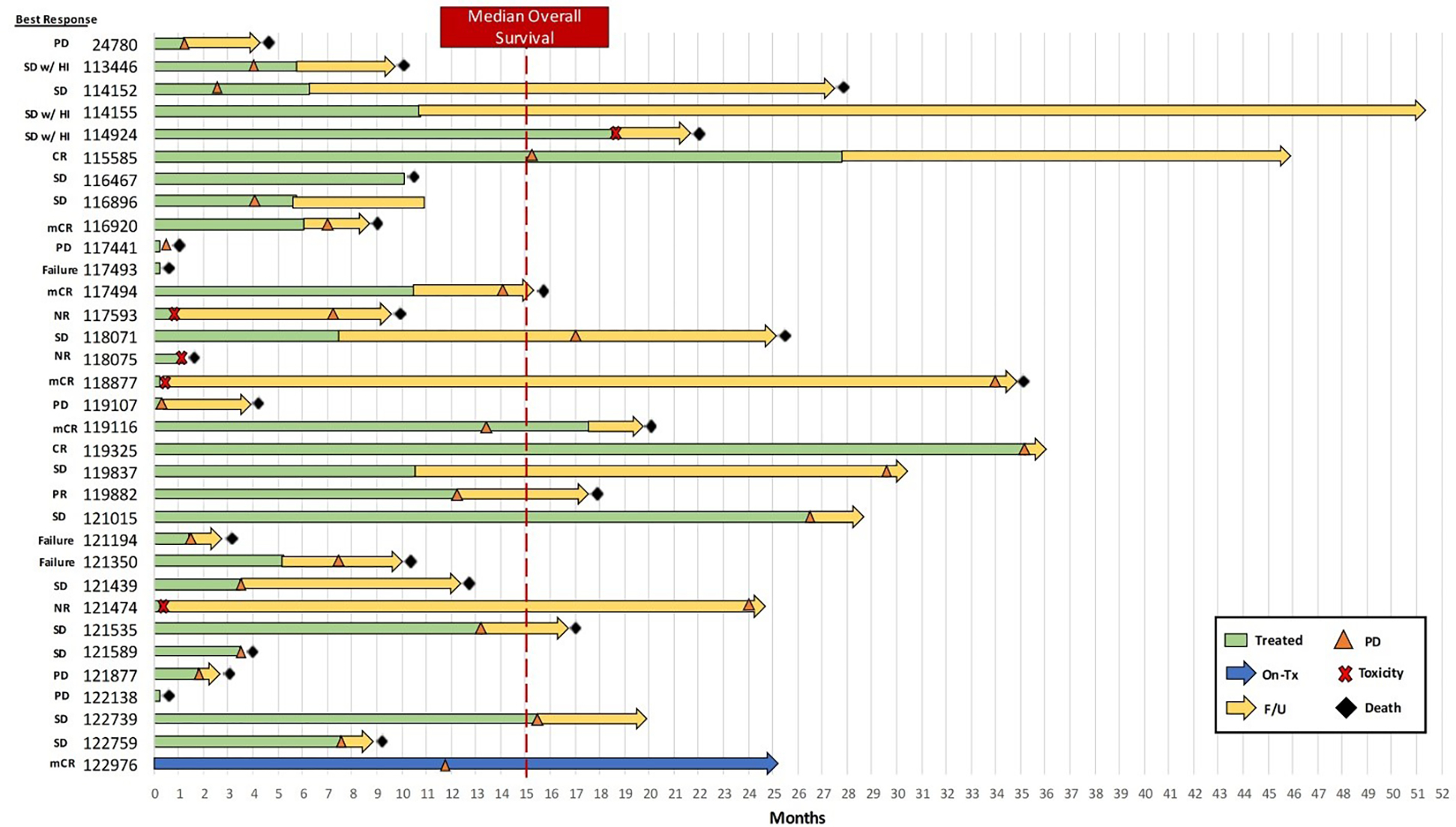
Results: Thirty-three patients, median age 73 (range 54-85), were treated. Thirty patients had MDS and 3 had CMML, with 30% relapsed and 70% refractory. No dose-limiting toxicities were observed in Phase I. There were 3 (9%) deaths in ≤ 30 days. Five patients (16%) came off study for drug-related toxicity. Immune-related adverse events (IRAE) occurred in 12 (36%) patients (4 grade 3, 3 grade 2, and 5 grade1). ORR was 33% [95% confidence interval (CI), 19%-52%] with 2 complete remission (CR), 3 hematologic improvement, 5 marrow CR, and 1 partial remission. Median overall survival was 15.1 (95% CI, 8.5-25.3) months.
Conclusions: Guadecitabine with atezolizumab has modest efficacy with manageable IRAEs and typical cytopenia-related safety concerns for patients with relapsed or refractory MDS and CMML.
©2022 American Association for Cancer Research.
Conflict of interest statement
Conflict-of-interest disclosure: CO: Prior research support from Astex Pharmaceuticals, Inc. JWH: Honorarium from Bristol-Meyer Squibb. AE: Research grants: Jazz Pharmaceuticals, NewLink Genetics, Amgen and Servier, Global oncology advisory board member: Amgen, Advisory board member: Genentech, Servier, Kite Pharma, Consultant: Secura Bio, Co-Founders and Scientific Advisor: KinaRx, Inc. SRH: is the cofounder PokeAcell and is the co-inventor of the patents WO2015185067 and WO2015188839 for the barcoded MHC technology which is licenced to Immudex and co-inventor of the licensed patent for Combination encoding of MHC multimers (EP2088/009356), licensee: Sanquin, NL. PJ: Consultant, Zymo Corporation. MRB, ADØ, SKS, VHD, PK, DTW, HSJ, SHT, JC, BTB, KH, RB, GH, BAY, JPI, SBB, IS, KG: The authors declare no potential conflict of interest.
Figures
References
-
- Volpe VO, Garcia-Manero G, Komrojki RS. Myelodysplastic syndromes : A new decade. Clin Lymphoma Myeloma Leuk 2021;22(1):1–16. - PubMed
-
- Duong VH, Lin K, Reljic T, et al. Poor outcome of patient with myelodysplastic syndrome after azacitidine treatment failure. Clin Lymphoma Myeloma Leuk 2013;13(6):711–5. - PubMed
-
- Ørskov AD, Grønbæk K. DNA methyltransferase inhibitors in myeloid cancer: Clonal eradication or clonal differentiation. Cancer Journal 2017;23(5):277–285. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
