

Prehospital predictors of the need for transfusion in patients with major trauma
- PMID: 36222858
- PMCID: PMC10175474
- DOI: 10.1007/s00068-022-02132-5
Prehospital predictors of the need for transfusion in patients with major trauma
Abstract
Purpose: Severe haemorrhage is a leading cause of early mortality following major trauma. By early identification of patients at risk, blood transfusion could already be initiated in the prehospital period. Aim of the study was to evaluate the extent to which prehospital lactate and base excess, which are known to be associated with trauma-induced coagulopathy, and additional clinical parameters are associated with the need for early transfusion.
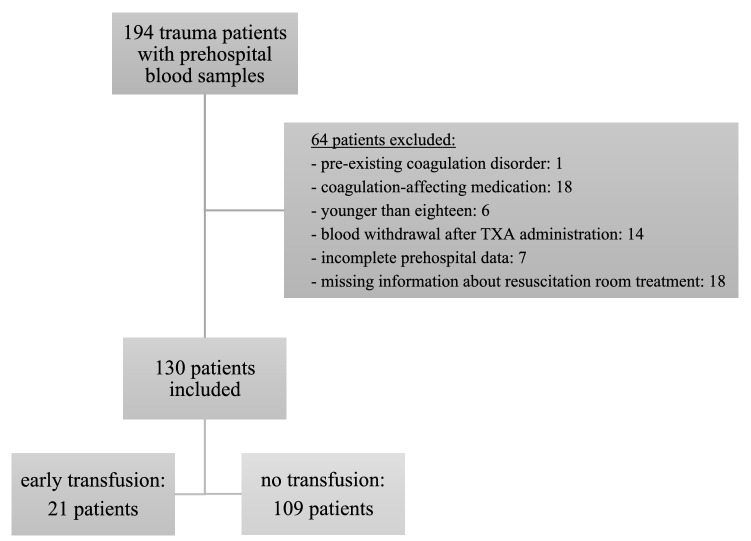
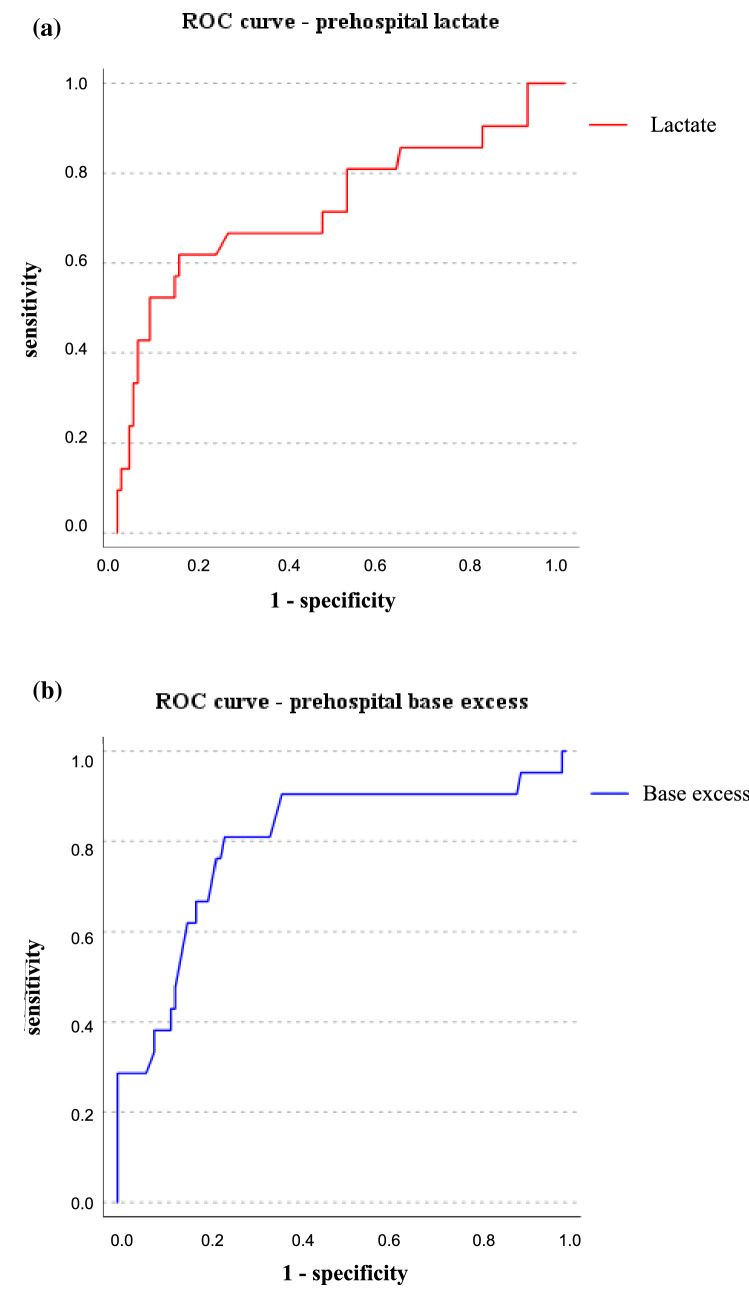
Methods: In this prospective, single-centre observational study, trauma patients treated by a helicopter emergency medical service were included, regardless of the injury severity. Patients with coagulation-influencing drugs in long-term therapy were excluded. Blood samples obtained at the beginning of the prehospital treatment were analysed. Primary outcome was the association of lactate and base excess with the need for early transfusion (resuscitation room or immediate surgery). Receiver operating characteristic curves were created, and the area under the curve (AUROC) was calculated.
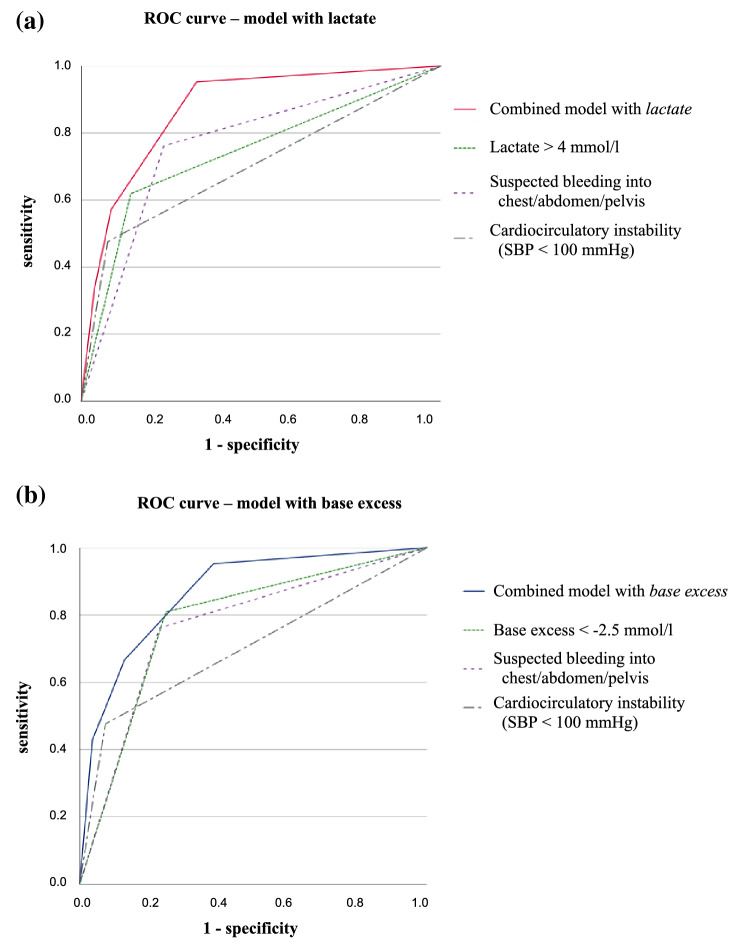
Results: Between 2015 and 2018, 21 out of 130 adult trauma patients received blood products during the early in-hospital treatment. Both prehospital lactate and base excess were associated with the transfusion (AUROC 0.731 and 0.798, respectively). The optimal calculated cut-off values were 4 mmol/l (lactate) and - 2.5 mmol/l (base excess). When circulatory instability and suspected relevant bleeding were included, the association further improved (AUROC 0.871 and 0.866, respectively).
Conclusion: Prehospital lactate and base excess could be used in combination with other clinical parameters as indicators of the need for early transfusion. This relationship has yet to be confirmed in the current validation study.
Trial registration: German Clinical Trials Register, www.drks.de (No. DRKS 00009559).
Keywords: Blood gas analysis; Blood transfusion; Emergency medical services; Haemorrhage; Trauma.
© 2022. The Author(s).
Conflict of interest statement
Martin Kulla has received research grants from the German Interdisciplinary Association of Critical Care and Emergency Medicine, research grants from the German Federal Ministry of Education and Research, and personal fees from Boehringer Ingelheim Pharma GmbH & Co.KG (all outside the published topic). All other authors declare that they have no conflicts of interest.
Figures
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- Heron M. Deaths: leading causes for 2017. Natl Vital Stat Rep. 2019;68:1–77. - PubMed
-
- Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations and therapeutic considerations. J Trauma. 2006;60:S3–11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
