

Differences in Cancer Screening Responses to State Medicaid Expansions by Race and Ethnicity, 2011‒2019
- PMID: 36223588
- PMCID: PMC9558180
- DOI: 10.2105/AJPH.2022.307027
Differences in Cancer Screening Responses to State Medicaid Expansions by Race and Ethnicity, 2011‒2019
Abstract
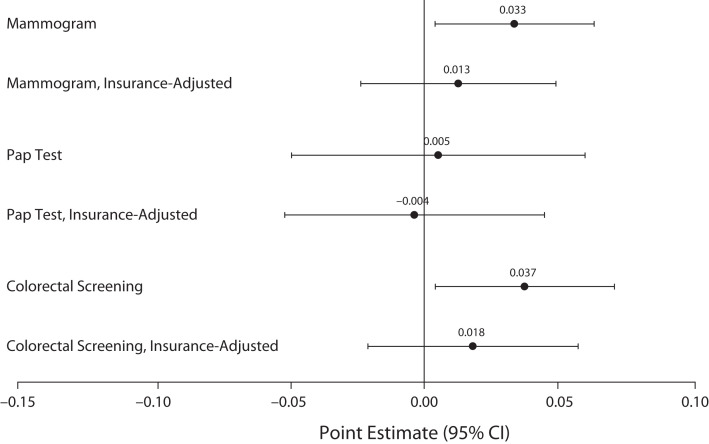
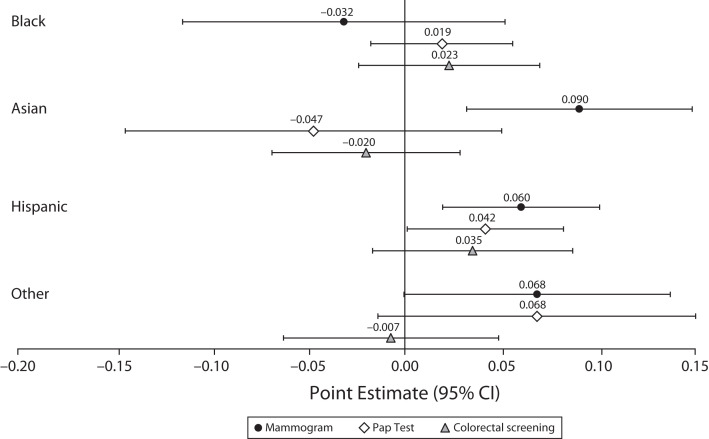
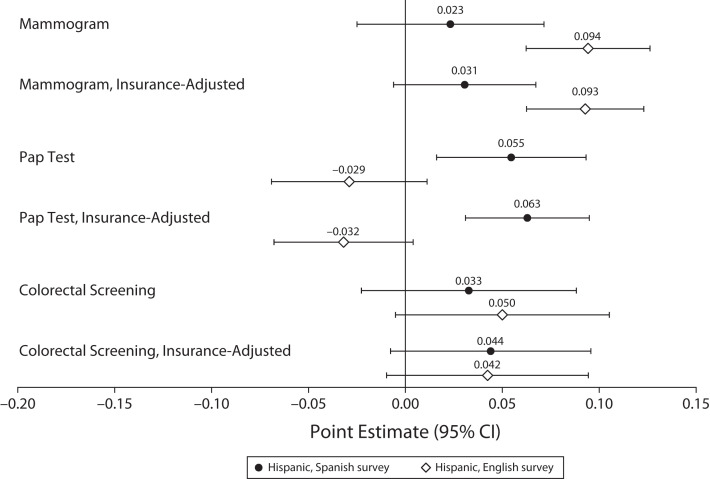
Objectives. To estimate whether state Medicaid expansions' relationships to breast, cervical, and colorectal cancer screening differ by race/ethnicity. Methods. Analyses conducted in 2021 used 2011-2016 and 2018-2019 Behavioral Risk Factor Surveillance System data on adults aged 40 to 64 years with household incomes below 400% of the federal poverty guideline (FPG; n = 537 250). Triple-difference analyses compared cancer screening in Medicaid expansion versus nonexpansion states, before versus after expansion, among people with incomes above versus below the eligibility cutoff (138% FPG). Race/ethnicity and ethnicity-by-language interaction terms tested for effect modification. Results. Associations between Medicaid expansions and cancer screening were significant for past-2-year mammograms and past-5-year colorectal screening. Effect modification analyses showed elevated mammography among non-Hispanic Asian women (+9.0 percentage points; 95% confidence interval [CI] = 3.2, 14.8) and Hispanic women (+6.0 percentage points; 95% CI = 2.0, 10.1), and Papanicolaou tests among Hispanic women (+4.2 percentage points; 95% CI = 0.1, 8.2). Findings were not limited to English- or Spanish-speaking respondents and were robust to insurance status controls. Conclusions. Medicaid expansions yielded statistically significant increases in income-eligible Asian and Hispanic women's mammography and Hispanic women's Pap testing relative to non-Hispanic White women. Neither language proficiency nor insurance status explained these findings. (Am J Public Health. 2022;112(11):1630-1639. https://doi.org/10.2105/AJPH.2022.307027).
Figures
Similar articles
-
Surveillance for Health Care Access and Health Services Use, Adults Aged 18-64 Years - Behavioral Risk Factor Surveillance System, United States, 2014.MMWR Surveill Summ. 2017 Feb 24;66(7):1-42. doi: 10.15585/mmwr.ss6607a1. MMWR Surveill Summ. 2017. PMID: 28231239 Free PMC article.
-
State Medicaid expansion decisions and disparities in women's cancer screening.Am J Prev Med. 2015 Jan;48(1):98-103. doi: 10.1016/j.amepre.2014.08.015. Epub 2014 Oct 30. Am J Prev Med. 2015. PMID: 25441234 Free PMC article.
-
Health Reform, Medicaid Expansions, and Women's Cancer Screening.Womens Health Issues. 2016 May-Jun;26(3):256-61. doi: 10.1016/j.whi.2016.01.002. Epub 2016 Feb 23. Womens Health Issues. 2016. PMID: 26926159
-
The Impacts of the ACA Medicaid Expansions on Cancer Screening Use by Primary Care Provider Supply.Med Care. 2019 Mar;57(3):202-207. doi: 10.1097/MLR.0000000000001053. Med Care. 2019. PMID: 30624303
-
Early Coverage, Access, Utilization, and Health Effects Associated With the Affordable Care Act Medicaid Expansions: A Quasi-experimental Study.Ann Intern Med. 2016 Jun 21;164(12):795-803. doi: 10.7326/M15-2234. Epub 2016 Apr 19. Ann Intern Med. 2016. PMID: 27088438 Free PMC article.
Cited by
-
Preventive Care Needs of the North Carolina Medicaid Expansion Population.AJPM Focus. 2024 Oct 18;4(1):100289. doi: 10.1016/j.focus.2024.100289. eCollection 2025 Feb. AJPM Focus. 2024. PMID: 39628936 Free PMC article.
-
Cervical Cancer Screening Among Female Medicaid Beneficiaries With and Without Schizophrenia.Schizophr Bull. 2024 Nov 8;50(6):1499-1507. doi: 10.1093/schbul/sbae096. Schizophr Bull. 2024. PMID: 38842724 Free PMC article.
-
Assessing impact of a community-based screening campaign to address social determinants of cervical cancer.JNCI Cancer Spectr. 2025 Jan 3;9(1):pkaf006. doi: 10.1093/jncics/pkaf006. JNCI Cancer Spectr. 2025. PMID: 39888858 Free PMC article.
References
-
- Curry SJ, Byers T, Hewitt ME. Fulfilling the Potential of Cancer Prevention and Early Detection. Washington, DC: National Academies Press; 2003. National Cancer Policy Board. Potential of screening to reduce the burden of cancer. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
