

The effect of the surgical approach and cochlear implant electrode on the structural integrity of the cochlea in human temporal bones
- PMID: 36224234
- PMCID: PMC9556579
- DOI: 10.1038/s41598-022-21399-7
The effect of the surgical approach and cochlear implant electrode on the structural integrity of the cochlea in human temporal bones
Abstract
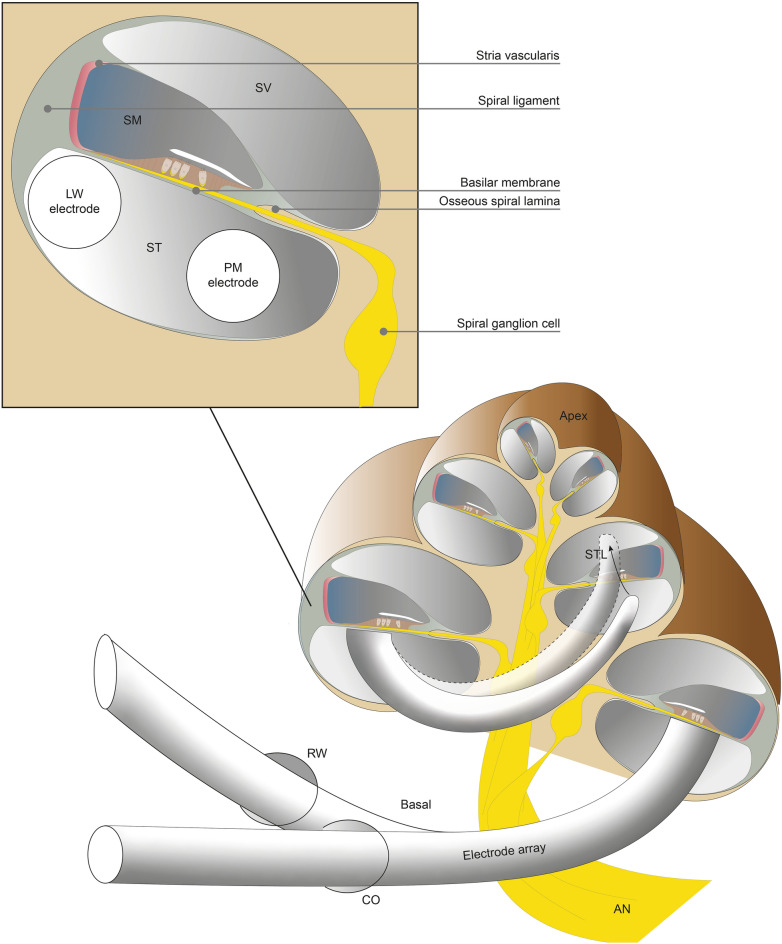
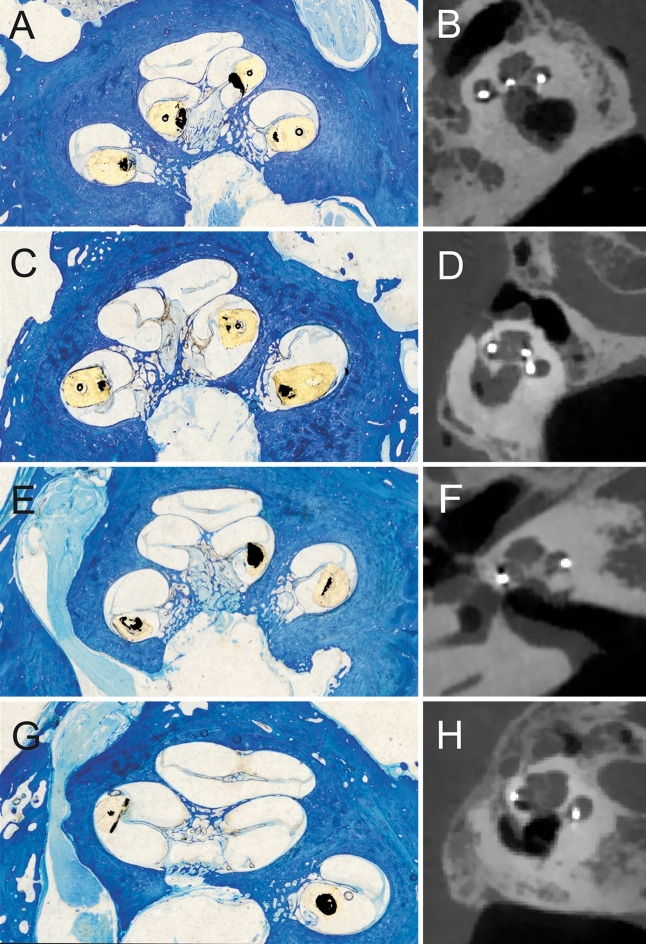
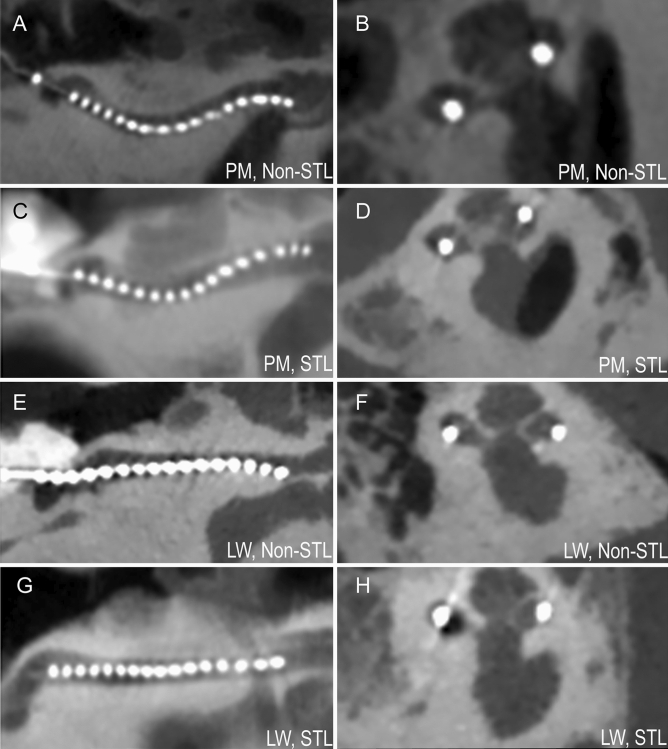
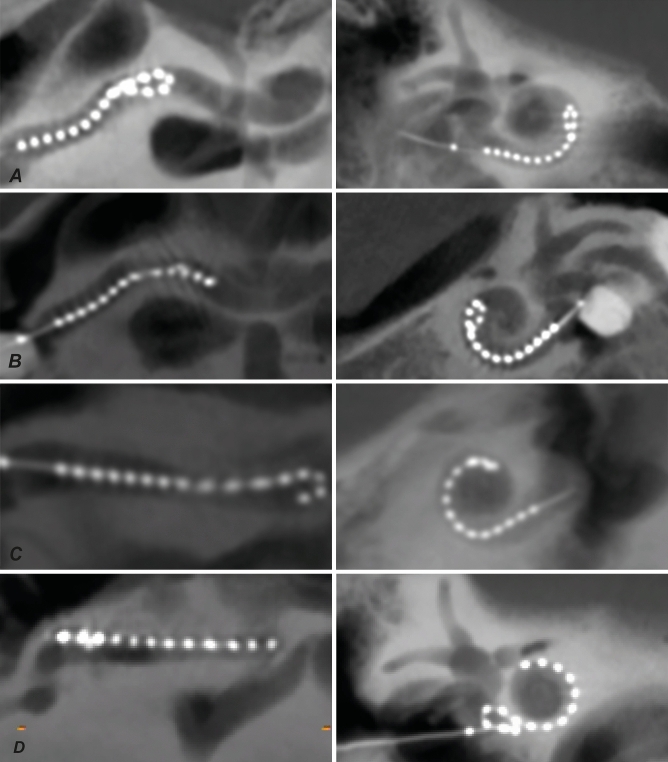
Cochlear implants (CI) restore hearing of severely hearing-impaired patients. Although this auditory prosthesis is widely considered to be very successful, structural cochlear trauma during cochlear implantation is an important problem, reductions of which could help to improve hearing outcomes and to broaden selection criteria. The surgical approach in cochlear implantation, i.e. round window (RW) or cochleostomy (CO), and type of electrode-array, perimodiolar (PM) or lateral wall (LW), are variables that might influence the probability of severe trauma. We investigated the effect of these two variables on scalar translocation (STL), a specific type of severe trauma. Thirty-two fresh frozen human cadaveric ears were evenly distributed over four groups receiving either RW or CO approach, and either LW or PM array. Conventional radiological multiplanar reconstruction (MPR) was compared with a reconstruction method that uncoils the spiral shape of the cochlea (UCR). Histological analysis showed that RW with PM array had STL rate of 87% (7/8), CO approach with LW array 75% (6/8), RW approach with LW array 50% (4/8) and CO approach with PM array 29% (2/7). STL assessment using UCR showed a higher inter-observer and histological agreement (91 and 94% respectively), than that using MPR (69 and 74% respectively). In particular, LW array positions were difficult to assess with MPR. In conclusion, the interaction between surgical approach and type of array should be preoperatively considered in cochlear implant surgery. UCR technique is advised for radiological assessment of CI positions, and in general it might be useful for pathologies involving the inner ear or other complex shaped bony tubular structures.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





Similar articles
-
Evaluating cochlear insertion trauma and hearing preservation after cochlear implantation (CIPRES): a study protocol for a randomized single-blind controlled trial.Trials. 2021 Dec 9;22(1):895. doi: 10.1186/s13063-021-05878-2. Trials. 2021. PMID: 34886884 Free PMC article.
-
Impact of electrode design and surgical approach on scalar location and cochlear implant outcomes.Laryngoscope. 2014 Nov;124 Suppl 6(0 6):S1-7. doi: 10.1002/lary.24728. Epub 2014 May 30. Laryngoscope. 2014. PMID: 24764083 Free PMC article.
-
Does cochleostomy location influence electrode trajectory and intracochlear trauma?Laryngoscope. 2015 Apr;125(4):966-71. doi: 10.1002/lary.24986. Epub 2014 Oct 27. Laryngoscope. 2015. PMID: 25345671
-
Cochlear implant electrode insertion: in defence of cochleostomy and factors against the round window membrane approach.Cochlear Implants Int. 2011 Aug;12 Suppl 2:S36-9. doi: 10.1179/146701011X13074645127478. Cochlear Implants Int. 2011. PMID: 21917217 Review.
-
An overview of cochlear implant electrode array designs.Hear Res. 2017 Dec;356:93-103. doi: 10.1016/j.heares.2017.10.005. Epub 2017 Oct 18. Hear Res. 2017. PMID: 29102129 Review.
Cited by
-
Acute effects of cochleostomy and electrode-array insertion on compound action potentials in normal-hearing guinea pigs.Front Neurosci. 2023 Feb 8;17:978230. doi: 10.3389/fnins.2023.978230. eCollection 2023. Front Neurosci. 2023. PMID: 36845413 Free PMC article.
-
Cochlear implant electrode design for safe and effective treatment.Front Neurol. 2024 May 2;15:1348439. doi: 10.3389/fneur.2024.1348439. eCollection 2024. Front Neurol. 2024. PMID: 38756216 Free PMC article. Review.
-
The role of pressure and friction forces in automated insertion of cochlear implants.Front Neurol. 2024 Aug 6;15:1430694. doi: 10.3389/fneur.2024.1430694. eCollection 2024. Front Neurol. 2024. PMID: 39170077 Free PMC article.
-
Models of Cochlea Used in Cochlear Implant Research: A Review.Ann Biomed Eng. 2023 Jul;51(7):1390-1407. doi: 10.1007/s10439-023-03192-3. Epub 2023 Apr 22. Ann Biomed Eng. 2023. PMID: 37087541 Free PMC article. Review.
-
Intracochlear Trauma and Local Ossification Patterns Differ Between Straight and Precurved Cochlear Implant Electrodes.Otol Neurotol. 2024 Mar 1;45(3):245-255. doi: 10.1097/MAO.0000000000004102. Epub 2024 Jan 17. Otol Neurotol. 2024. PMID: 38270168 Free PMC article.
References
-
- Gifford RH, Revit LJ. Speech perception for adult cochlear implant recipients in a realistic background noise: Effectiveness of preprocessing strategies and external options for improving speech recognition in noise. J. Am. Acad. Audiol. 2010;21:441–451. doi: 10.3766/jaaa.21.7.3. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
