

Exploring the association between cognitive decline and all-cause mortality with blood pressure as a potential modifier in oldest old individuals
- PMID: 36224279
- PMCID: PMC9556626
- DOI: 10.1038/s41598-022-21487-8
Exploring the association between cognitive decline and all-cause mortality with blood pressure as a potential modifier in oldest old individuals
Abstract
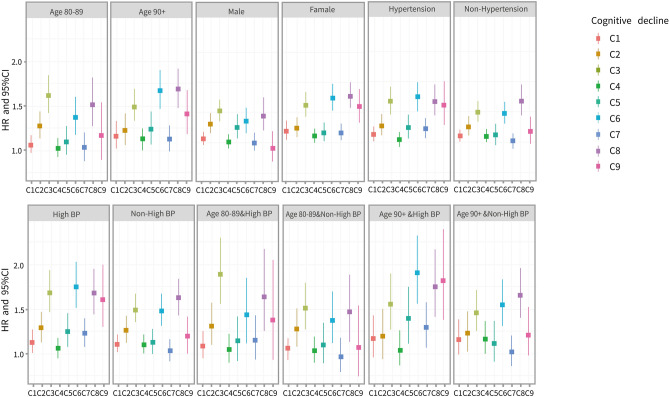
Few studies have systematically explored the association between cognitive decline and all-cause mortality among oldest old individuals (above 80 years old), and there is limited evidence of blood pressure (BP) as a potential effect modifier. Therefore, this study included 14,891 oldest old individuals (mean age: 90.3 ± 7.5 years); 10,904 deaths and 34,486 person-years were observed. Cognitive scores were calculated using the Chinese version of the Mini-Mental State Examination (MMSE). Cognitive decline was stratified into ten categories (C0-C9). Continuous cognitive scores were used to assess the interactions of modifiers of the cognitive decline and all-cause mortality association and potentially modifiable factors. Potential effect modifiers were explored by age, sex, BP status and hypertension. Cox proportional hazards models were used to evaluate the relationship between cognitive decline and all-cause mortality after adjustments for demographic characteristics, socioeconomic status, lifestyle factors, leisure activities and health conditions. Participants who progressed to severe cognitive impairment from high normal cognitive function (C3), low normal cognitive function (C6), or mild cognitive impairment (C8) had 55%, 56%, and 63% higher mortality risks, respectively, than those who maintained high normal cognitive function (C0). The multivariate-adjusted model indicated that oldest old individuals with a decrease of more than one point in the MMSE score per year had an approximately 4% all-cause mortality risk. The relationship between cognitive decline and mortality was statistically influenced by sex (P = 0.013), high BP in nonagenarians (P = 0.003), and hypertension (P = 0.004) but not by age (P = 0.277). Our findings suggest that periodic screening for cognitive decline and strengthening BP management may be necessary for public health.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Association between dietary diversity and cognitive impairment among the oldest-old: Findings from a nationwide cohort study.Clin Nutr. 2021 Apr;40(4):1452-1462. doi: 10.1016/j.clnu.2021.02.041. Epub 2021 Mar 2. Clin Nutr. 2021. PMID: 33740515
-
Adherence to High Dietary Diversity and Incident Cognitive Impairment for the Oldest-Old: A Community-Based, Nationwide Cohort Study.Nutrients. 2022 Oct 27;14(21):4530. doi: 10.3390/nu14214530. Nutrients. 2022. PMID: 36364792 Free PMC article.
-
Lower blood pressure during antihypertensive treatment is associated with higher all-cause mortality and accelerated cognitive decline in the oldest-old. Data from the Leiden 85-plus Study.Age Ageing. 2018 Jul 1;47(4):545-550. doi: 10.1093/ageing/afy072. Age Ageing. 2018. PMID: 29741555
-
Evaluation of Intensive vs Standard Blood Pressure Reduction and Association With Cognitive Decline and Dementia: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Nov 1;4(11):e2134553. doi: 10.1001/jamanetworkopen.2021.34553. JAMA Netw Open. 2021. PMID: 34807261 Free PMC article.
-
Effects of Antihypertensive Drugs on Cognitive Function in Elderly Patients with Hypertension: A Review.Aging Dis. 2021 Jun 1;12(3):841-851. doi: 10.14336/AD.2020.1111. eCollection 2021 Jun. Aging Dis. 2021. PMID: 34094646 Free PMC article. Review.
Cited by
-
Is Formal Social Participation Associated with Cognitive Function in Middle-Aged and Older Adults? A Systematic Review with Meta-Analysis of Longitudinal Studies.Behav Sci (Basel). 2024 Mar 22;14(4):262. doi: 10.3390/bs14040262. Behav Sci (Basel). 2024. PMID: 38667058 Free PMC article. Review.
-
Effect of blood pressure on mortality in patients with cognitive impairment: a prospective cohort study.Front Cardiovasc Med. 2023 Dec 12;10:1282131. doi: 10.3389/fcvm.2023.1282131. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 38155982 Free PMC article.
-
Effect of glucose variability on the mortality of adults aged 75 years and over during the first year of the COVID-19 pandemic.BMC Geriatr. 2024 Jun 20;24(1):533. doi: 10.1186/s12877-024-05149-0. BMC Geriatr. 2024. PMID: 38902647 Free PMC article.
-
2023 Guideline for the management of hypertension in the elderly population in China.J Geriatr Cardiol. 2024 Jun 28;21(6):589-630. doi: 10.26599/1671-5411.2024.06.001. J Geriatr Cardiol. 2024. PMID: 38973827 Free PMC article. No abstract available.
-
What factors preventing the older adults in China from living longer: a machine learning study.BMC Geriatr. 2024 Jul 22;24(1):625. doi: 10.1186/s12877-024-05214-8. BMC Geriatr. 2024. PMID: 39039463 Free PMC article.
References
-
- Leng X, Espeland MA, Manson JE, Stefanick ML, Gower EW, Hayden KM, Limacher MC, Vaughan L, Robinson J, Wallace R, et al. Cognitive function and changes in cognitive function as predictors of incident cardiovascular disease: The Women's Health Initiative Memory Study. J. Gerontol. A Biol. Sci. Med. Sci. 2018;73(6):779–785. doi: 10.1093/gerona/glx138. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
