

Glioblastoma, IDH-wildtype with leptomeningeal metastasis to Meckel's cave: A case report
- PMID: 36225898
- PMCID: PMC9549091
- DOI: 10.1177/20584601221131480
Glioblastoma, IDH-wildtype with leptomeningeal metastasis to Meckel's cave: A case report
Abstract
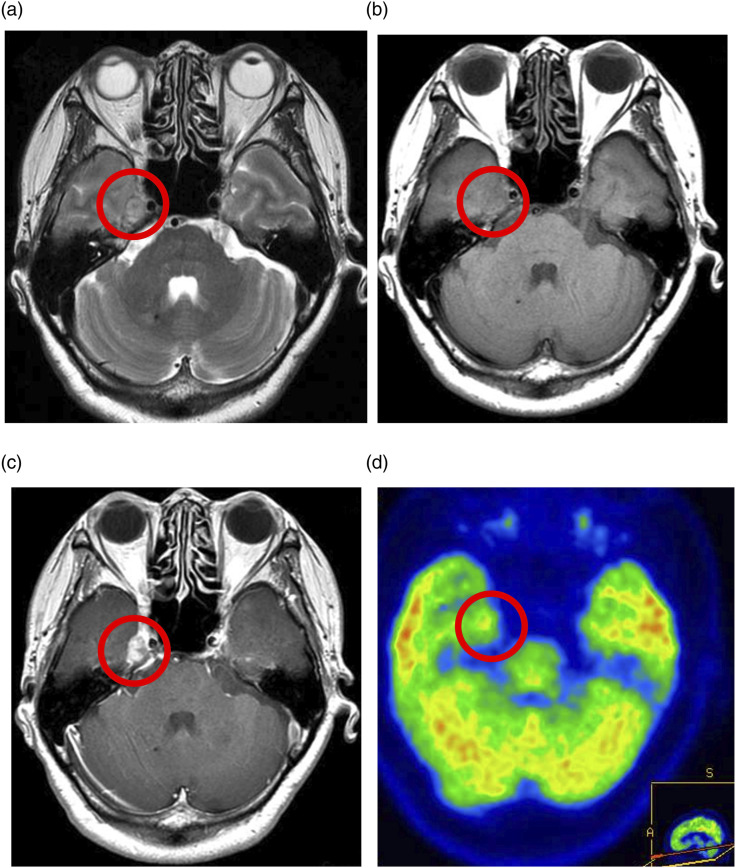
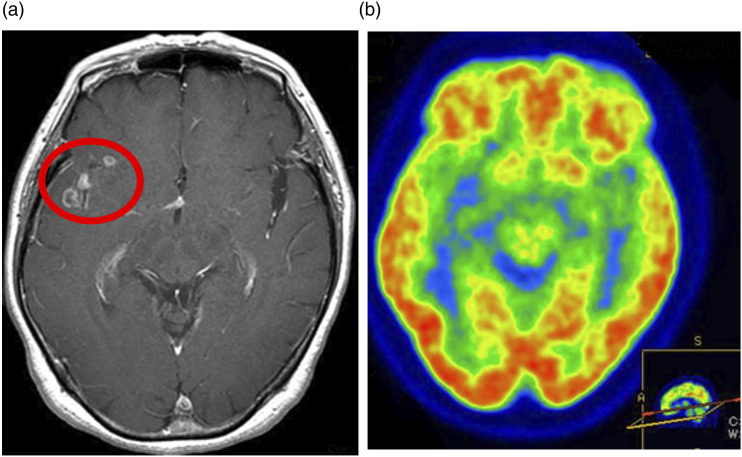
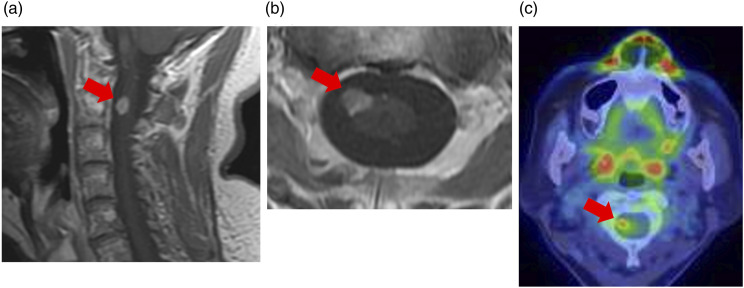
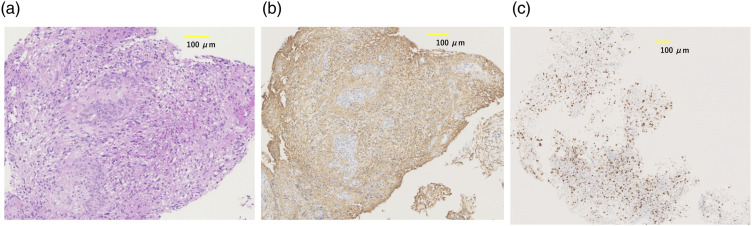
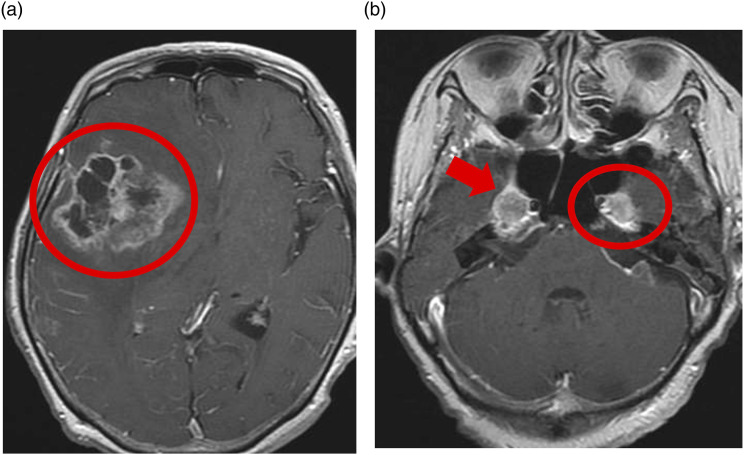
Meckel's cave or the trigeminal cistern is a subarachnoid space near the apex of the petrous portion of the temporal bone and contains cerebrospinal fluid and the Gasserian ganglion, which divides into the ophthalmic (V1), maxillary (V2), and mandibular (V3) nerves. Infectious, inflammatory, congenital, and neoplastic lesions can occur in Meckel's cave. Leptomeningeal metastasis of glioblastoma (GBM), IDH-wildtype to Meckel's cave is rare. We encountered a case of leptomeningeal metastasis of GBM to Meckel's cave in an elderly female patient who presented with pain around her right eye. Magnetic resonance imaging revealed enhancing lesions in the right temporal lobe and cervical spinal cord. The pathological diagnosis of GBM was confirmed after biopsy of the cervical spinal cord lesion, which showed hyperaccumulation of fluorodeoxyglucose (FDG) on FDG-positron emission tomography. This case indicates that metastatic lesions can also occur in Meckel's cave.
Keywords: FDG-PET; IDH-wildtype; Meckel’s cave; glioblastoma; leptomeningeal metastasis.
© The Author(s) 2022.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Trigeminal Neuropathy.2024 Mar 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 32310586 Free Books & Documents.
-
Distant metastasis of hepatocellular carcinoma to Meckel's cave and cranial nerves: A case report and review of literature.World J Hepatol. 2021 Jun 27;13(6):709-716. doi: 10.4254/wjh.v13.i6.709. World J Hepatol. 2021. PMID: 34239705 Free PMC article.
-
Neuroimaging of Meckel's cave in normal and disease conditions.Insights Imaging. 2018 Aug;9(4):499-510. doi: 10.1007/s13244-018-0604-7. Epub 2018 Apr 18. Insights Imaging. 2018. PMID: 29671218 Free PMC article. Review.
-
An Alternative Endoscopic Anterolateral Route to Meckel's Cave: An Anatomic Feasibility Study Using a Sublabial Transmaxillary Approach.World Neurosurg. 2018 Jun;114:134-141. doi: 10.1016/j.wneu.2018.02.128. Epub 2018 Mar 3. World Neurosurg. 2018. PMID: 29510274
-
Prepontine and Meckel's Cave Dermoid Cyst: MR and CT Findings with Literature Review.J Coll Physicians Surg Pak. 2022 Apr;32(4):525-527. doi: 10.29271/jcpsp.2022.04.525. J Coll Physicians Surg Pak. 2022. PMID: 35330530 Review.
Cited by
-
Trigeminal nerve-driven neurogenic inflammation linking migraine to glioblastoma invasion: a literature review.Front Immunol. 2025 Jul 16;16:1632154. doi: 10.3389/fimmu.2025.1632154. eCollection 2025. Front Immunol. 2025. PMID: 40740778 Free PMC article. Review.
References
-
- Chetan RS, Gyanendra K, Pradeep S, et al. Metastases to Meckel's cave: report of two cases and comparative analysis of malignant tumors with meningioma and schwannoma of Meckel's cave. Clin Neurol Neurosurg 2010; 112: 927–932. - PubMed
-
- Ashwani K, Donald WC, Ernesto B. The Meckel cave: computed tomographic study. Part I: normal anatomy; Part II: Pathology. Radiology 1984; 152: 425–433. - PubMed
-
- Benjamin K, Errol MB. The trigeminal nerve cistern. Radiology 1973; 108: 597–602. - PubMed
-
- VandeVyver V, Lemmerling M, Van Hecke W, et al. MRI findings of the normal and diseased trigeminal nerve ganglion and branches a pictorial review. JBR-BTR 2007; 90: 272–277. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
