

Comparison of Efficacy and Safety Between Laparoscopic and Open Radical Resection for Hilar Cholangiocarcinoma-A Propensity Score-Matching Analysis
- PMID: 36226051
- PMCID: PMC9549331
- DOI: 10.3389/fonc.2022.1004974
Comparison of Efficacy and Safety Between Laparoscopic and Open Radical Resection for Hilar Cholangiocarcinoma-A Propensity Score-Matching Analysis
Abstract
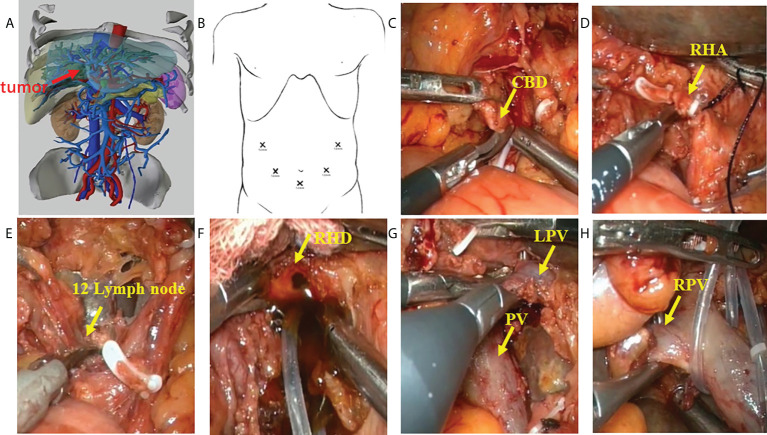
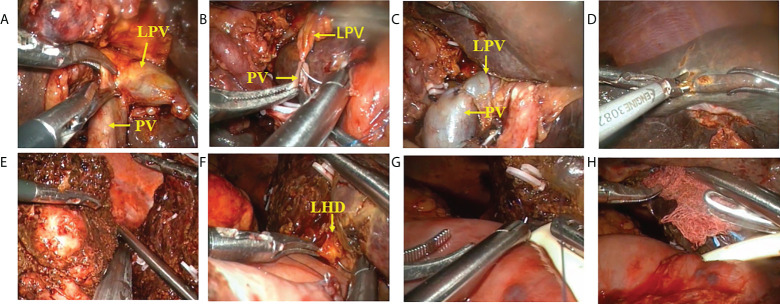
Background: Radical resection remains the most effective treatment for hilar cholangiocarcinoma (HCCA). However, due to the complex anatomy of the hilar region, the tumor is prone to invade portal vein and hepatic arteries, making the surgical treatment of HCCA particularly difficult. Successful laparoscopic radical resection of HCCA(IIIA, IIIB) requires excellent surgical skills and rich experience. Furthermore, the safety and effectiveness of this operation are still controversial.
Aim: To retrospectively analyze and compare the efficacy and safety of laparoscopic and open surgery for patients with HCCA.
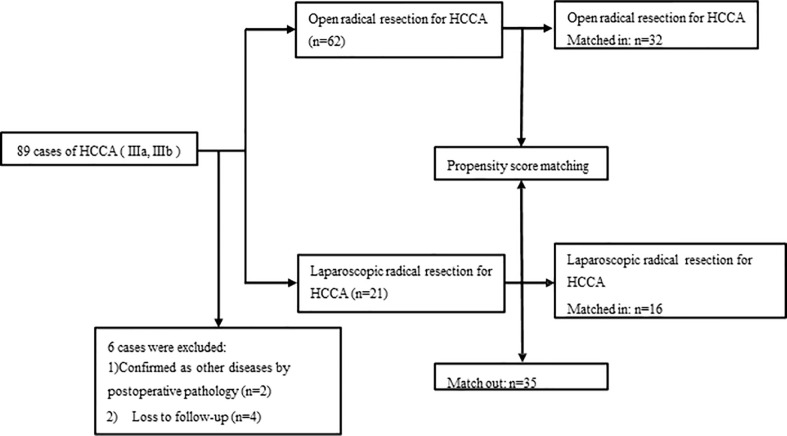
Methods: Clinical imaging and postoperative pathological data of 89 patients diagnosed with HCCA (IIIA, IIIB) and undergoing radical resection in our center from January 2018 to March 2022 were retrospectively analyzed. Among them, 6 patients (4 were lost to follow-up and 2 were pathologically confirmed to have other diseases after surgery) were ruled out, and clinical data was collected from the remaining 83 patients for statistical analysis. These patients were divided into an open surgery group (n=62) and a laparoscopic surgery group (n=21) according to the surgical methods used, and after 1:2 propensity score matching (PSM), 32 and 16 patients respectively in the open surgery group and laparoscopic surgery group were remained. The demographic data, Bismuth type, perioperative data, intraoperative data, postoperative complications, pathological findings, and long-term survivals were compared between these two groups.
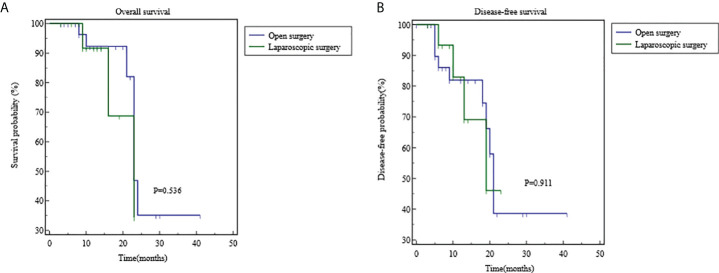
Results: After 1:2 PSM, 32 patients in the open surgery group and 16 patients in the laparoscopic surgery group were included for further analysis. Baseline characteristics and pathological outcomes were comparable between the two groups. Statistically significant differences between the two groups were observed in intraoperative blood loss and operative time, as it were 400-800 mL vs 200-400 mL (P=0.012) and (407.97 ± 76.06) min vs (489.69 ± 79.17) min (P=0.001) in the open surgery group and laparoscopic surgery group, respectively. The R0 resection rate of the open group was 28 cases (87.5%), and the R0 resection rate of the laparoscopic group was 15 cases (93.75%). The two groups showed no significant difference in terms of surgical approach, intraoperative blood transfusion, incidence of postoperative complications, and short- and long-term efficacy (P>0.05).
Conclusions: Laparoscopic radical resection of HCCA has comparable perioperative safety compared to open surgery group, as it has less bleeding and shorter operation time. Although it is a promising procedure with the improvement of surgical skills and further accumulation of experience, further investigations are warranted before its wider application.
Keywords: R0 resection; laparoscopic hilar cholangiocarcinoma; open hilar cholangiocarcinoma; propensity score matching; retrospective study.
Copyright © 2022 He, Huang, Ren, Li, Yang, Deng, Li, Peng, Tang, Zheng, Huang and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Evaluation of the outcomes of biliary-enteric reconstruction in robotic radical resection of hilar cholangiocarcinoma: a single-center propensity score matching analysis.Sci Rep. 2024 Jun 27;14(1):14836. doi: 10.1038/s41598-024-65875-8. Sci Rep. 2024. PMID: 38937559 Free PMC article.
-
Total laparoscopic versus open radical resection for hilar cholangiocarcinoma.Surg Endosc. 2020 Oct;34(10):4382-4387. doi: 10.1007/s00464-019-07211-0. Epub 2019 Oct 29. Surg Endosc. 2020. PMID: 31664578
-
"Hepatic hilum area priority, liver posterior first": An optimized strategy in laparoscopic resection for type III-IV hilar cholangiocarcinoma.World J Gastrointest Surg. 2024 Jul 27;16(7):2167-2174. doi: 10.4240/wjgs.v16.i7.2167. World J Gastrointest Surg. 2024. PMID: 39087123 Free PMC article.
-
A Consensus Meeting on Expert Recommendations on Operating Specifications for Laparoscopic Radical Resection of Hilar Cholangiocarcinoma.Front Surg. 2021 Nov 23;8:731448. doi: 10.3389/fsurg.2021.731448. eCollection 2021. Front Surg. 2021. PMID: 34888342 Free PMC article.
-
Surgical Strategies for the Treatment of Bismuth Type I and II Hilar Cholangiocarcinoma: Bile Duct Resection with or Without Hepatectomy?Ann Surg Oncol. 2020 Sep;27(9):3374-3382. doi: 10.1245/s10434-020-08453-2. Epub 2020 Apr 9. Ann Surg Oncol. 2020. PMID: 32274664
Cited by
-
Safety and feasibility of laparoscopic radical resection for bismuth types III and IV hilar cholangiocarcinoma: a single-center experience from China.Front Oncol. 2023 Dec 18;13:1280513. doi: 10.3389/fonc.2023.1280513. eCollection 2023. Front Oncol. 2023. PMID: 38188306 Free PMC article.
-
Minimally Invasive Surgery for Perihilar Cholangiocarcinoma: A Systematic Review of the Short- and Long-Term Results.Cancers (Basel). 2023 Jun 3;15(11):3048. doi: 10.3390/cancers15113048. Cancers (Basel). 2023. PMID: 37297010 Free PMC article. Review.
-
Short- and long-term outcomes of laparoscopic versus open resection of perihilar cholangiocarcinoma: a propensity score-based analysis.Hepatobiliary Surg Nutr. 2025 Apr 1;14(2):207-221. doi: 10.21037/hbsn-23-680. Epub 2024 Aug 12. Hepatobiliary Surg Nutr. 2025. PMID: 40342757 Free PMC article.
-
Risk Factors for Negative Emotions in Patients Undergoing Radical Resection of Hilar Cholangiocarcinoma and Their Influence on Prognosis.Int J Gen Med. 2023 Dec 11;16:5841-5853. doi: 10.2147/IJGM.S440469. eCollection 2023. Int J Gen Med. 2023. PMID: 38106978 Free PMC article.
-
Efficacy and Safety of Robotic Surgery vs. Open Surgery for Hilar Cholangiocarcinoma: A Comprehensive Review.Cureus. 2024 Aug 13;16(8):e66790. doi: 10.7759/cureus.66790. eCollection 2024 Aug. Cureus. 2024. PMID: 39268261 Free PMC article. Review.
References
-
- Nuzzo G, Giuliante F, Ardito F, Giovannini I, Aldrighetti L, Belli G, et al. . Improvement in perioperative and long-term outcome after surgical treatment of hilar cholangiocarcinoma: Results of an Italian multicenter analysis of 440 patients. Arch Surg (2012) 147(1):26–34. doi: 10.1001/archsurg.2011.771 - DOI - PubMed
-
- Coelen RJ, Olthof PB, van Dieren S, Besselink MG, Busch OR, van Gulik TM. External validation of the estimation of physiologic ability and surgical stress (E-PASS) risk model to predict operative risk in perihilar cholangiocarcinoma. JAMA Surg (2016) 151(12):1132–8. doi: 10.1001/jamasurg.2016.2305 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous