

Accelerating integration of tobacco use treatment in the context of lung cancer screening: Relevance and application of implementation science to achieving policy and practice
- PMID: 36227937
- PMCID: PMC9677484
- DOI: 10.1093/tbm/ibac076
Accelerating integration of tobacco use treatment in the context of lung cancer screening: Relevance and application of implementation science to achieving policy and practice
Abstract
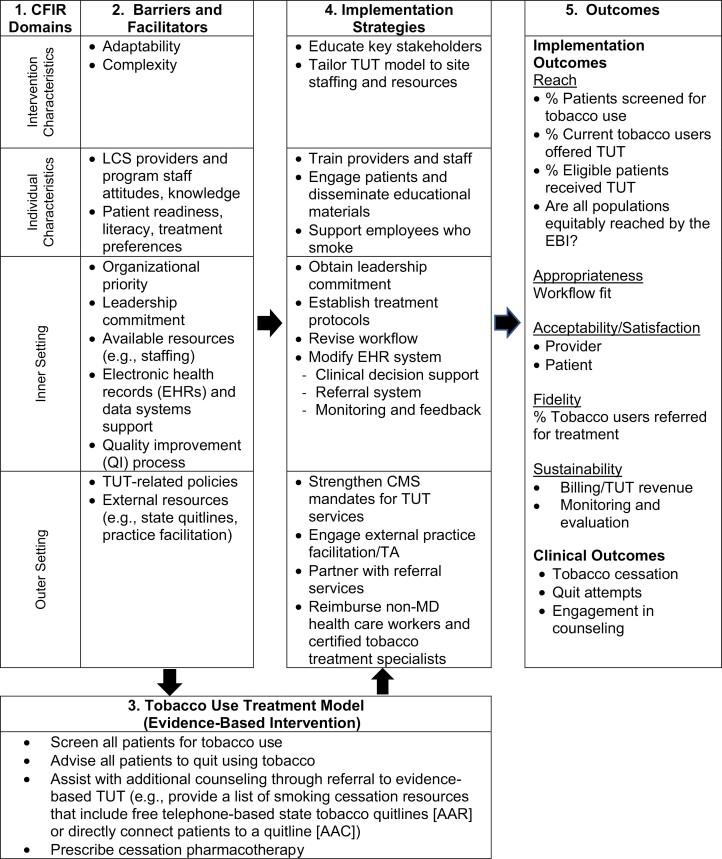
Based on the findings from the National Lung Screening Trial, the U.S. Preventive Services Task Force recommends annual low dose computed tomography (LDCT) lung cancer screening (LCS) among high-risk adults. Approximately 54% of individuals seeking LCS report current cigarette smoking. Effective smoking cessation interventions, offered at the time of LCS, enhances the health benefits of screening that are attributable to reductions in lung cancer overall and tobacco-related mortality. Considering these data, the Centers for Medicare & Medicaid Services' (CMS) 2015 decision to cover LCS with LDCT required that radiology imaging facilities make tobacco cessation interventions available for people who smoke. In February 2022, CMS reversed their 2015 coverage requirement for delivering tobacco use treatment at the time of LDCT; CMS retained the requirement for counseling during the shared decision-making visit prior to the exam. The policy change does not diminish the importance of offering high-quality tobacco cessation services in conjunction with routine LDCT for LCS. However, LCS programs face a range of barriers to implementing tobacco use treatment in their settings. As a result, implementation has lagged. Closing the "evidence to practice" gap is the focus of implementation science, a field that offers a set of rigorous methods and a systematic approach to identifying and overcoming contextual barriers to implementing evidence-based guidelines in a range of clinical settings. In this paper, we describe how implementation science frameworks and methods can be used to help guide LCS programs in their efforts to integrate tobacco use treatment and discuss policy changes needed to further facilitate the delivery of TUT as an essential component of the LCS process.
Keywords: Implementation science; Lung cancer screening; Tobacco cessation; Tobacco use treatment.
Plain language summary
Lung cancer is the leading cause of cancer death in the United States. There is strong evidence, from a large number of international studies, that lung cancer screening for people who meet specific criteria, can reduce lung cancer-related deaths. Based on these findings, the Centers for Medicare and Medicaid decided to provide insurance coverage for lung cancer screening for eligible patients. This includes people aged 50–80 years who have a 20 pack-year smoking history and currently smoke or have quit within the past 15 years. Over 50% of people who seek lung cancer screening report current cigarette smoking. Studies show that offering these smokers support to quit at the time of screening can further increase survival rates by reducing both deaths from lung cancer and other tobacco-related diseases. Unfortunately, lung cancer screening programs do not consistently provide effective treatments to help smokers quit. This is a missed opportunity to engage smokers in quitting when the health risk of tobacco use is most salient, and therefore smokers may be more willing to engage in tobacco use treatment. This paper provides detailed guidance on how programs can implement high quality tobacco use treatment services in conjunction with lung cancer screening.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Society of Behavioral Medicine.
Figures
Similar articles
-
Pairing smoking-cessation services with lung cancer screening: A clinical guideline from the Association for the Treatment of Tobacco Use and Dependence and the Society for Research on Nicotine and Tobacco.Cancer. 2016 Apr 15;122(8):1150-9. doi: 10.1002/cncr.29926. Epub 2016 Feb 24. Cancer. 2016. PMID: 26916412 Free PMC article. Review.
-
A protocol for a cluster randomized trial of care delivery models to improve the quality of smoking cessation and shared decision making for lung cancer screening.Contemp Clin Trials. 2023 May;128:107141. doi: 10.1016/j.cct.2023.107141. Epub 2023 Mar 5. Contemp Clin Trials. 2023. PMID: 36878389 Free PMC article.
-
Study protocol of a multiphase optimization strategy trial (MOST) for delivery of smoking cessation treatment in lung cancer screening settings.Trials. 2022 Aug 17;23(1):664. doi: 10.1186/s13063-022-06568-3. Trials. 2022. PMID: 35978334 Free PMC article.
-
Screening for lung cancer: 2023 guideline update from the American Cancer Society.CA Cancer J Clin. 2024 Jan-Feb;74(1):50-81. doi: 10.3322/caac.21811. Epub 2023 Nov 1. CA Cancer J Clin. 2024. PMID: 37909877
-
The 10 Pillars of Lung Cancer Screening: Rationale and Logistics of a Lung Cancer Screening Program.Radiographics. 2015 Nov-Dec;35(7):1893-908. doi: 10.1148/rg.2015150079. Epub 2015 Oct 23. Radiographics. 2015. PMID: 26495797 Review.
Cited by
-
Budget impact analysis for implementation decision making, planning, and financing.Transl Behav Med. 2024 Jan 11;14(1):54-59. doi: 10.1093/tbm/ibad059. Transl Behav Med. 2024. PMID: 37776567 Free PMC article.
-
Tobacco treatment specialists' knowledge, attitudes and beliefs about lung cancer screening: Potential piece of the puzzle for increasing lung cancer screening awareness.Patient Educ Couns. 2023 Oct;115:107871. doi: 10.1016/j.pec.2023.107871. Epub 2023 Jun 29. Patient Educ Couns. 2023. PMID: 37437512 Free PMC article.
-
Expanding reach, enhancing capacity: embracing the role of primary care in lung cancer screening and smoking cessation in the United States.Lancet Reg Health Am. 2024 Aug 21;38:100870. doi: 10.1016/j.lana.2024.100870. eCollection 2024 Oct. Lancet Reg Health Am. 2024. PMID: 39253709 Free PMC article. No abstract available.
-
Barriers to Integrating Tobacco Dependence Treatment into Lung Cancer Screening: A Qualitative Assessment.J Prim Care Community Health. 2025 Jan-Dec;16:21501319251321608. doi: 10.1177/21501319251321608. J Prim Care Community Health. 2025. PMID: 39993144 Free PMC article.
-
Nurse-Led Tobacco Cessation for Veterans Using Motivational Interviewing in a Lung Cancer Screening Program.Clin J Oncol Nurs. 2025 Mar 14;29(2):130-134. doi: 10.1188/25.CJON.130-134. Clin J Oncol Nurs. 2025. PMID: 40096569 Free PMC article.
References
-
- United States Preventive Services Taskforce. Final Recommendation Statement—Lung Cancer: Screening; 2021. Rockville, MD: Author; 2021. Available at https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung.... Accessibility verified February 24, 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
