

Risk perception and subsidy policy-based voluntary vaccination driven by multiple information sources
- PMID: 36227953
- PMCID: PMC9560505
- DOI: 10.1371/journal.pone.0276177
Risk perception and subsidy policy-based voluntary vaccination driven by multiple information sources
Abstract
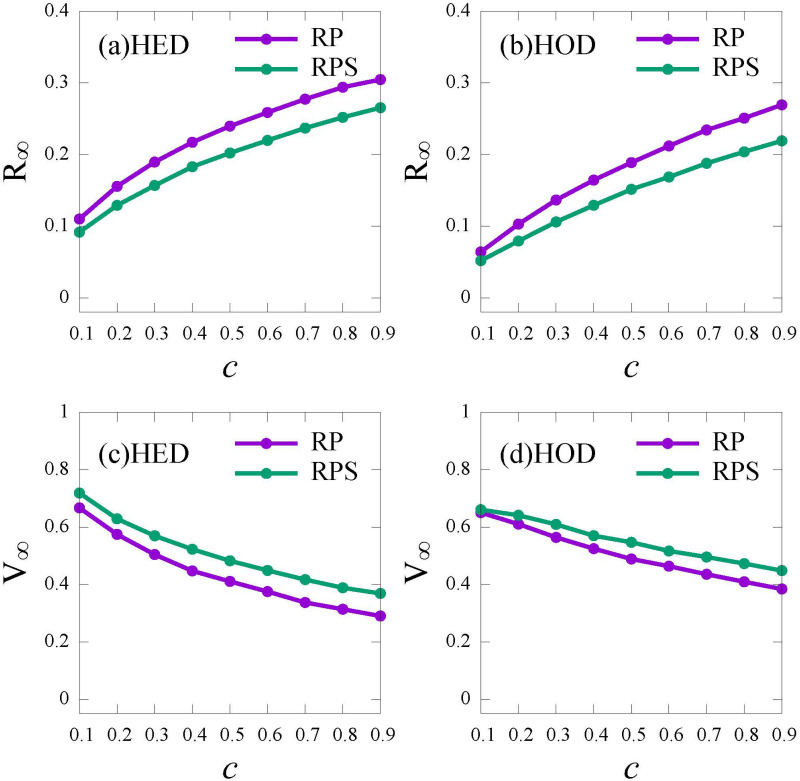
Exploring vaccination behavior is fundamental to understand the role of vaccine in suppressing the epidemic. Motivated by the efficient role of the risk perception and the subsidy policy in promoting vaccination, we propose the Risk Perception and the Risk Perception with Subsidy Policy voluntary vaccination strategies with imperfect vaccine. The risk perception is driven by multiple information sources based on global information (released by Public Health Bureau) and local information (from first-order neighbors). In time-varying networks, we use the mean-field approach and the Monte Carlo simulations to analyze the epidemic dynamics under vaccination behavior with imperfect vaccine. We find that vaccination with the incorporation of risk perception and subsidy policy can effectively control the epidemic. Moreover, information from different sources plays different roles. Global information is more helpful in promoting vaccination than local information. In addition, to further understand the influence of vaccination strategies, we calculate the social cost as the cost for the vaccine and treatment, and find that excess vaccination cost results in a higher social cost after the herd immunity. Thus, for balancing the epidemic control and social cost, providing individuals with more global information as well as local information would be helpful in vaccination. These results are expected to provide insightful guidance for designing the policy to promote vaccination.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures










Similar articles
-
Epidemic prevalence information on social networks can mediate emergent collective outcomes in voluntary vaccine schemes.PLoS Comput Biol. 2019 May 23;15(5):e1006977. doi: 10.1371/journal.pcbi.1006977. eCollection 2019 May. PLoS Comput Biol. 2019. PMID: 31120877 Free PMC article.
-
To vaccinate or not to vaccinate: A comprehensive study of vaccination-subsidizing policies with multi-agent simulations and mean-field modeling.J Theor Biol. 2019 May 21;469:107-126. doi: 10.1016/j.jtbi.2019.02.013. Epub 2019 Feb 23. J Theor Biol. 2019. PMID: 30807759
-
Voluntary vaccination dilemma with evolving psychological perceptions.J Theor Biol. 2018 Feb 14;439:65-75. doi: 10.1016/j.jtbi.2017.11.011. Epub 2017 Dec 13. J Theor Biol. 2018. PMID: 29199090
-
Vaccination and herd immunity: what more do we know?Curr Opin Infect Dis. 2012 Jun;25(3):243-9. doi: 10.1097/QCO.0b013e328352f727. Curr Opin Infect Dis. 2012. PMID: 22561998 Review.
-
Weighing the risks and benefits of vaccination.Adv Vet Med. 1999;41:701-13. doi: 10.1016/s0065-3519(99)80054-8. Adv Vet Med. 1999. PMID: 9890055 Review.
References
-
- Arenas A, Cota W, Gómez-Gardeñes J, Gómez S, Granell C, Matamalas JT, et al.. Modeling the spatiotemporal epidemic spreading of COVID-19 and the impact of mobility and social distancing interventions. Physical Review X. 2020;10(4):041055. doi: 10.1103/PhysRevX.10.041055 - DOI
-
- Bassolas A, Santoro A, Sousa S, Rognone S, Nicosia V. Optimising the mitigation of epidemic spreading through targeted adoption of contact tracing apps. Physical Review Research. 2022;4(2):023092. doi: 10.1103/PhysRevResearch.4.023092 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
