

Overall survival in the OlympiA phase III trial of adjuvant olaparib in patients with germline pathogenic variants in BRCA1/2 and high-risk, early breast cancer
- PMID: 36228963
- PMCID: PMC10207856
- DOI: 10.1016/j.annonc.2022.09.159
Overall survival in the OlympiA phase III trial of adjuvant olaparib in patients with germline pathogenic variants in BRCA1/2 and high-risk, early breast cancer
Abstract
Background: The randomized, double-blind OlympiA trial compared 1 year of the oral poly(adenosine diphosphate-ribose) polymerase inhibitor, olaparib, to matching placebo as adjuvant therapy for patients with pathogenic or likely pathogenic variants in germline BRCA1 or BRCA2 (gBRCA1/2pv) and high-risk, human epidermal growth factor receptor 2-negative, early breast cancer (EBC). The first pre-specified interim analysis (IA) previously demonstrated statistically significant improvement in invasive disease-free survival (IDFS) and distant disease-free survival (DDFS). The olaparib group had fewer deaths than the placebo group, but the difference did not reach statistical significance for overall survival (OS). We now report the pre-specified second IA of OS with updates of IDFS, DDFS, and safety.
Patients and methods: One thousand eight hundred and thirty-six patients were randomly assigned to olaparib or placebo following (neo)adjuvant chemotherapy, surgery, and radiation therapy if indicated. Endocrine therapy was given concurrently with study medication for hormone receptor-positive cancers. Statistical significance for OS at this IA required P < 0.015.
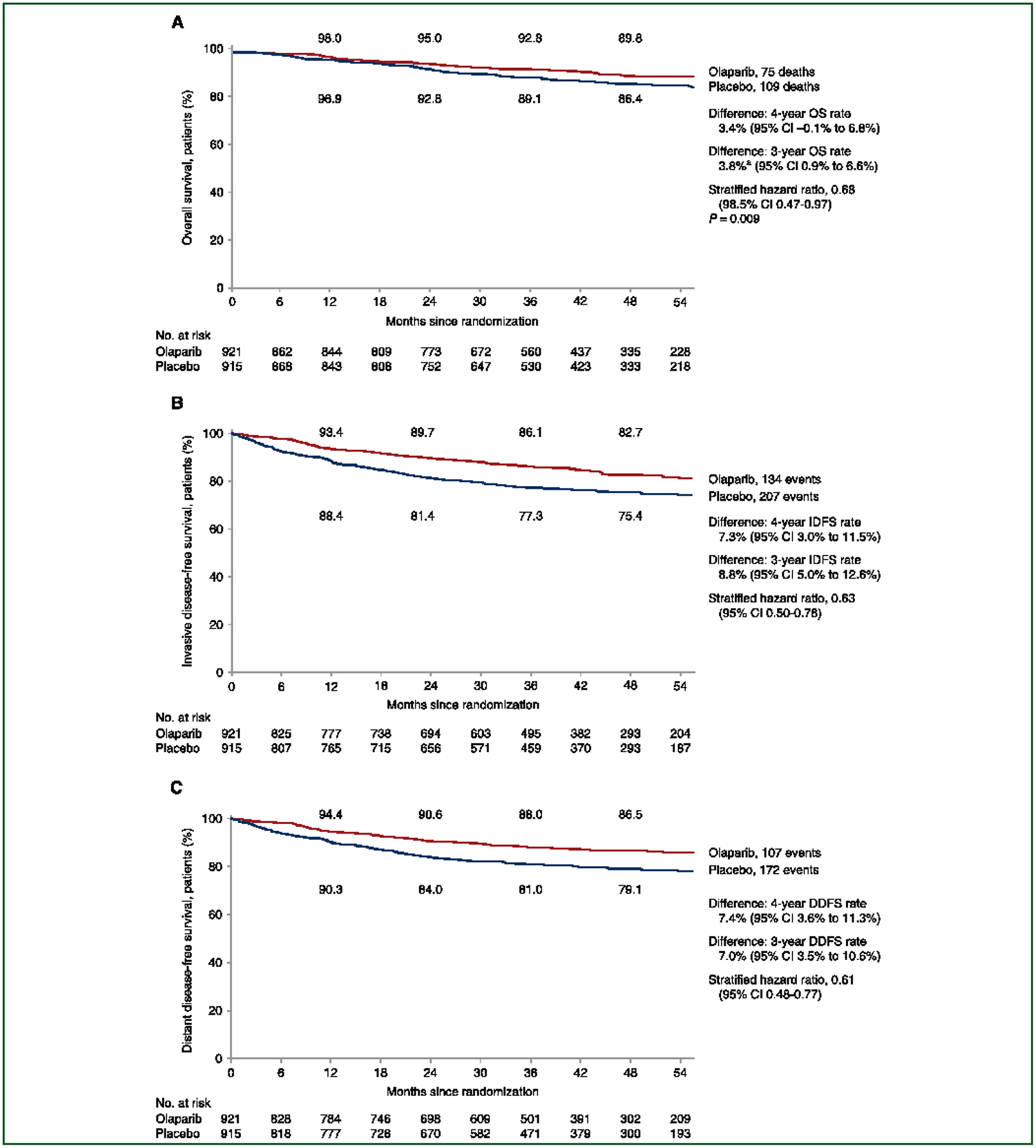
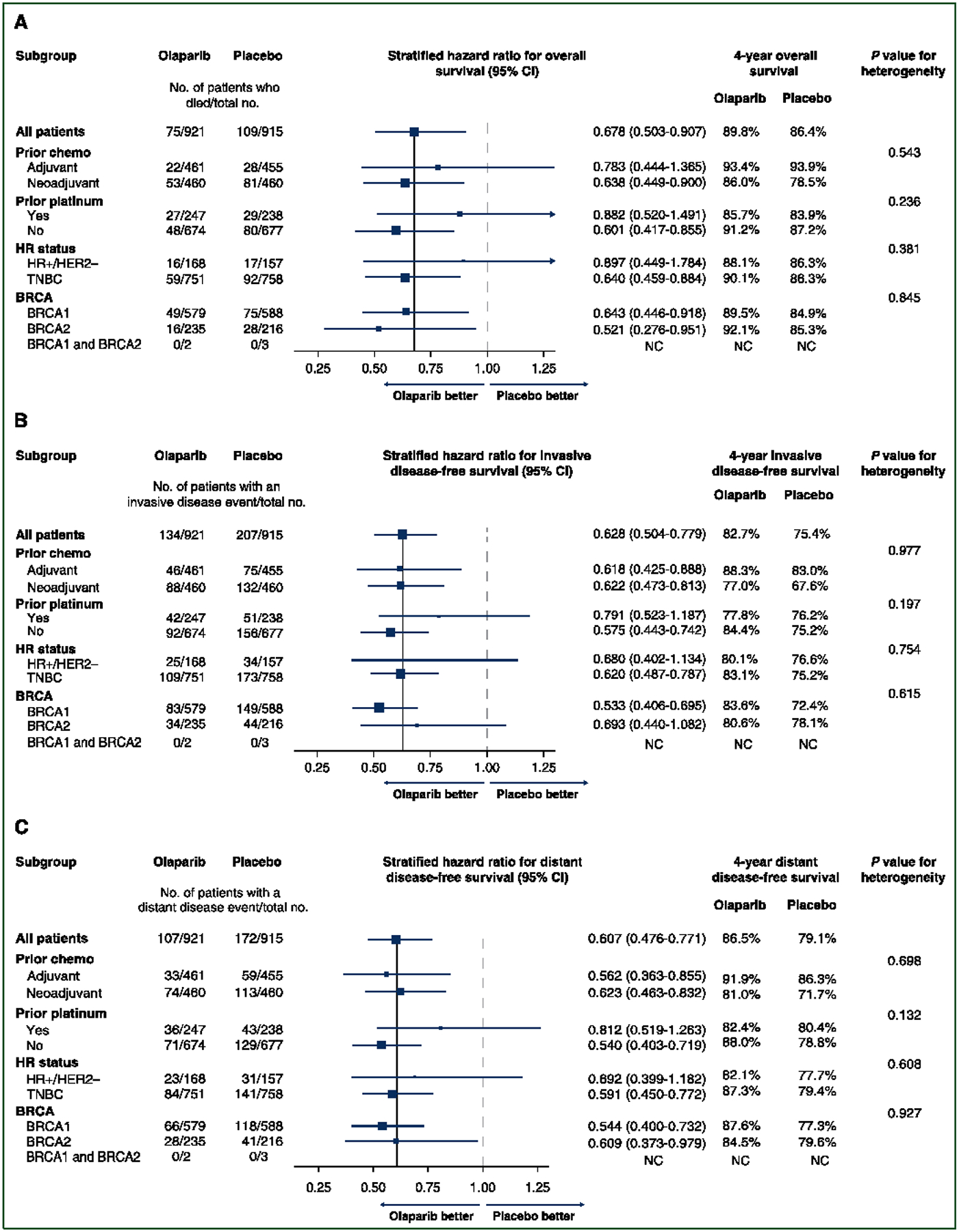
Results: With a median follow-up of 3.5 years, the second IA of OS demonstrated significant improvement in the olaparib group relative to the placebo group [hazard ratio 0.68; 98.5% confidence interval (CI) 0.47-0.97; P = 0.009]. Four-year OS was 89.8% in the olaparib group and 86.4% in the placebo group (Δ 3.4%, 95% CI -0.1% to 6.8%). Four-year IDFS for the olaparib group versus placebo group was 82.7% versus 75.4% (Δ 7.3%, 95% CI 3.0% to 11.5%) and 4-year DDFS was 86.5% versus 79.1% (Δ 7.4%, 95% CI 3.6% to 11.3%), respectively. Subset analyses for OS, IDFS, and DDFS demonstrated benefit across major subgroups. No new safety signals were identified including no new cases of acute myeloid leukemia or myelodysplastic syndrome.
Conclusion: With 3.5 years of median follow-up, OlympiA demonstrates statistically significant improvement in OS with adjuvant olaparib compared with placebo for gBRCA1/2pv-associated EBC and maintained improvements in the previously reported, statistically significant endpoints of IDFS and DDFS with no new safety signals.
Keywords: BRCA1/2; PARP inhibition; adjuvant therapy; breast cancer; olaparib.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Tutt A, Ashworth A. The relationship between the roles of BRCA genes in DNA repair and cancer predisposition. Trends Mol Med. 2002;8(12): 571–576. - PubMed
-
- Ashworth A. A synthetic lethal therapeutic approach: poly(ADP) ribose polymerase inhibitors for the treatment of cancers deficient in DNA double-strand break repair. J Clin Oncol. 2008;26(22):3785–3790. - PubMed
-
- Tutt ANJ, Lord CJ, McCabe N, et al. Exploiting the DNA repair defect in BRCA mutant cells in the design of new therapeutic strategies for cancer. Cold Spring Harb Symp Quant Biol. 2005;70:139–148. - PubMed
-
- Farmer H, McCabe N, Lord CJ, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature. 2005;434(7035): 917–921. - PubMed
-
- Robson M, Im SA, Senkus E, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N Engl J Med. 2017;377(6): 523–533. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
