

In critically ill patients, anti-anaerobic antibiotics increase risk of adverse clinical outcomes
- PMID: 36229047
- PMCID: PMC9909213
- DOI: 10.1183/13993003.00910-2022
In critically ill patients, anti-anaerobic antibiotics increase risk of adverse clinical outcomes
Abstract
Background: Critically ill patients routinely receive antibiotics with activity against anaerobic gut bacteria. However, in other disease states and animal models, gut anaerobes are protective against pneumonia, organ failure and mortality. We therefore designed a translational series of analyses and experiments to determine the effects of anti-anaerobic antibiotics on the risk of adverse clinical outcomes among critically ill patients.
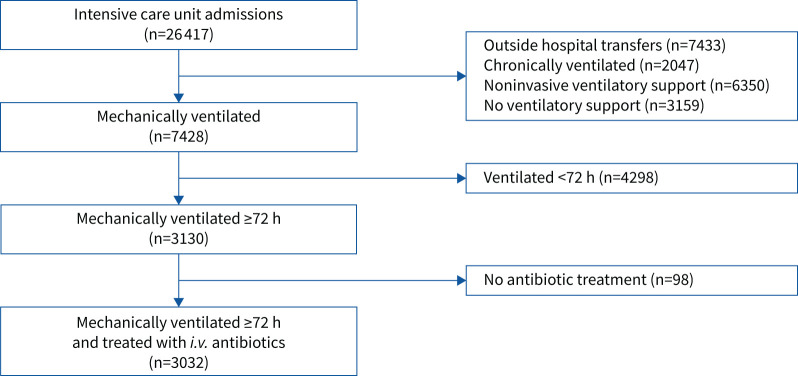
Methods: We conducted a retrospective single-centre cohort study of 3032 critically ill patients, comparing patients who did and did not receive early anti-anaerobic antibiotics. We compared intensive care unit outcomes (ventilator-associated pneumonia (VAP)-free survival, infection-free survival and overall survival) in all patients and changes in gut microbiota in a subcohort of 116 patients. In murine models, we studied the effects of anaerobe depletion in infectious (Klebsiella pneumoniae and Staphylococcus aureus pneumonia) and noninfectious (hyperoxia) injury models.
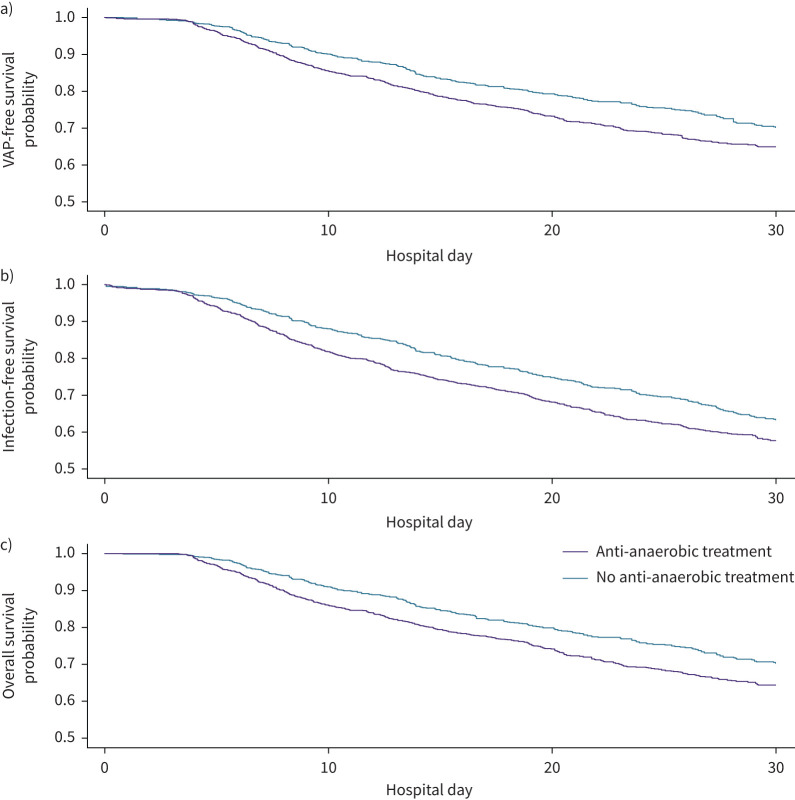
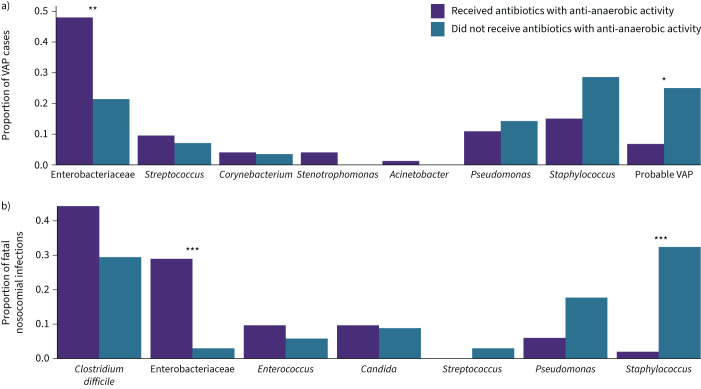
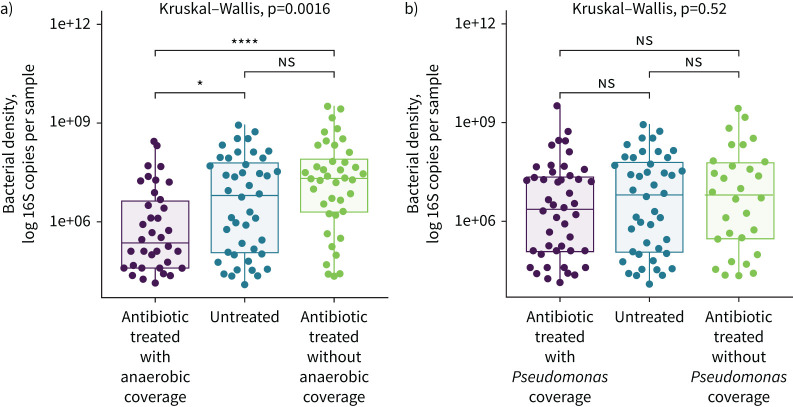
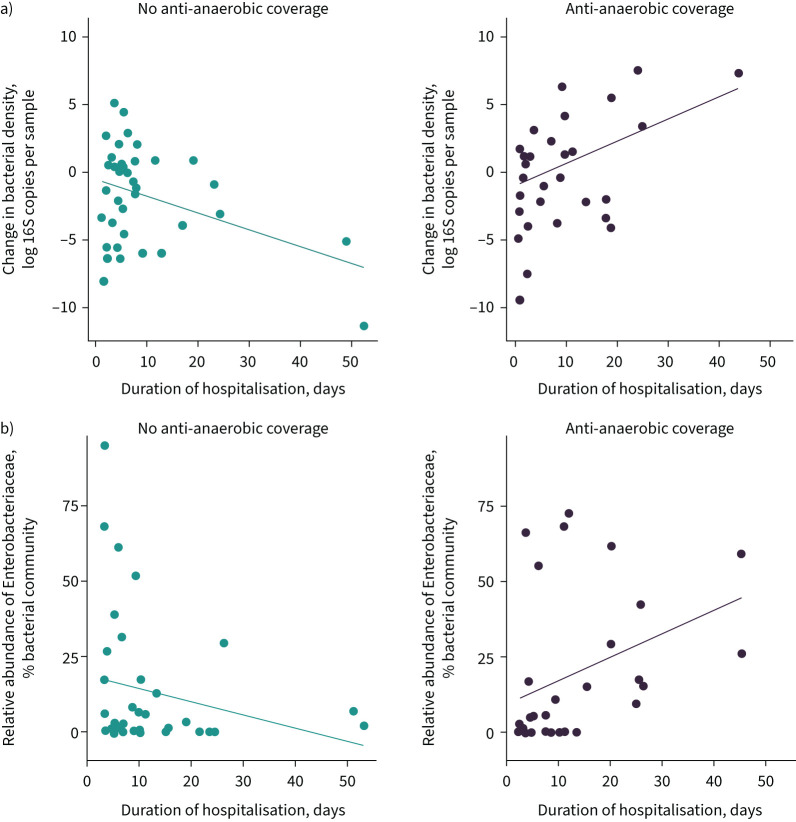
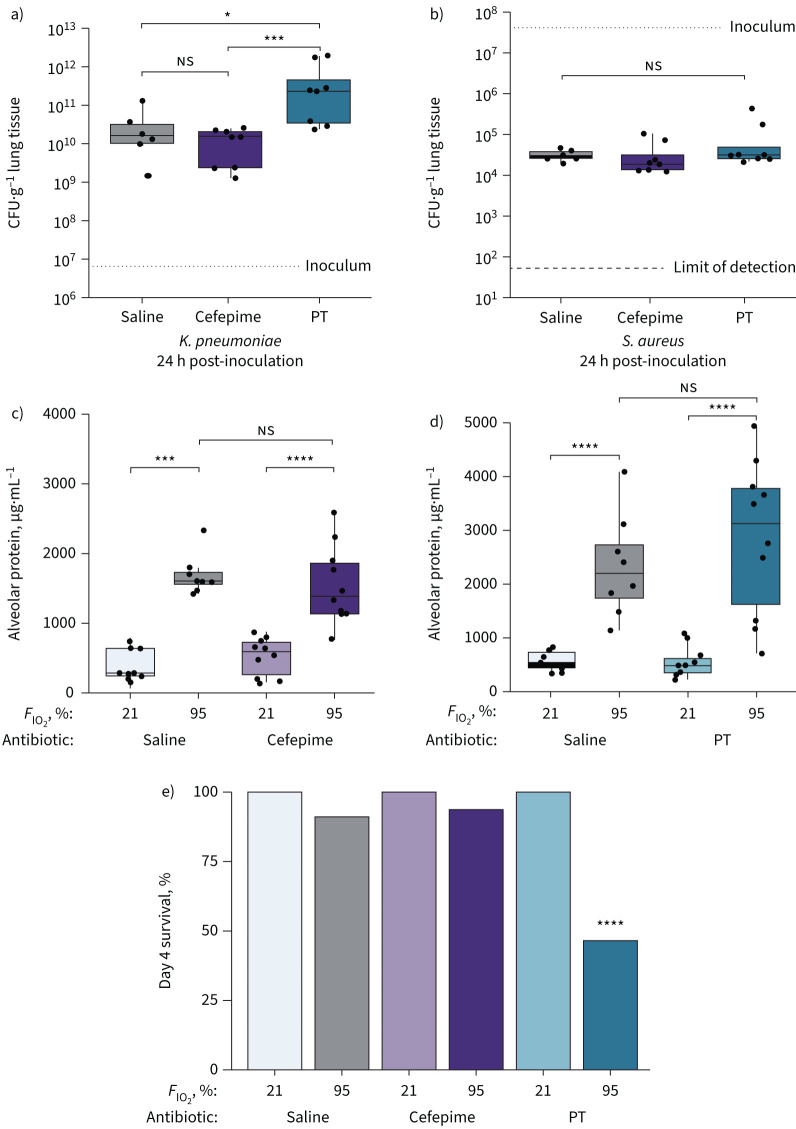
Results: Early administration of anti-anaerobic antibiotics was associated with decreased VAP-free survival (hazard ratio (HR) 1.24, 95% CI 1.06-1.45), infection-free survival (HR 1.22, 95% CI 1.09-1.38) and overall survival (HR 1.14, 95% CI 1.02-1.28). Patients who received anti-anaerobic antibiotics had decreased initial gut bacterial density (p=0.00038), increased microbiome expansion during hospitalisation (p=0.011) and domination by Enterobacteriaceae spp. (p=0.045). Enterobacteriaceae were also enriched among respiratory pathogens in anti-anaerobic-treated patients (p<2.2×10-16). In murine models, treatment with anti-anaerobic antibiotics increased susceptibility to Enterobacteriaceae pneumonia (p<0.05) and increased the lethality of hyperoxia (p=0.0002).
Conclusions: In critically ill patients, early treatment with anti-anaerobic antibiotics is associated with increased mortality. Mechanisms may include enrichment of the gut with respiratory pathogens, but increased mortality is incompletely explained by infections alone. Given consistent clinical and experimental evidence of harm, the widespread use of anti-anaerobic antibiotics should be reconsidered.
The content of this work is not subject to copyright. Design and branding are copyright ©ERS 2023.
Conflict of interest statement
Conflict of interest: All authors have nothing to disclose.
Figures

Comment in
-
Empiric anti-anaerobic antibiotics are associated with adverse clinical outcomes in emergency department patients.Eur Respir J. 2023 May 11;61(5):2300413. doi: 10.1183/13993003.00413-2023. Print 2023 May. Eur Respir J. 2023. PMID: 37169379 No abstract available.
-
Anti-anaerobic antibiotics: indication is key.Eur Respir J. 2023 May 11;61(5):2300318. doi: 10.1183/13993003.00318-2023. Print 2023 May. Eur Respir J. 2023. PMID: 37169380 No abstract available.
-
Reply to: Anti-anaerobic antibiotics: indication is key.Eur Respir J. 2023 May 11;61(5):2300492. doi: 10.1183/13993003.00492-2023. Print 2023 May. Eur Respir J. 2023. PMID: 37169381 No abstract available.
References
-
- Ewig S, Torres A, El-Ebiary M, et al. Bacterial colonization patterns in mechanically ventilated patients with traumatic and medical head injury. Incidence, risk factors, and association with ventilator-associated pneumonia. Am J Respir Crit Care Med 1999; 159: 188–198. doi: 10.1164/ajrccm.159.1.9803097 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous