

Tolerability and immunogenicity of an intranasally-administered adenovirus-vectored COVID-19 vaccine: An open-label partially-randomised ascending dose phase I trial
- PMID: 36229342
- PMCID: PMC9550199
- DOI: 10.1016/j.ebiom.2022.104298
Tolerability and immunogenicity of an intranasally-administered adenovirus-vectored COVID-19 vaccine: An open-label partially-randomised ascending dose phase I trial
Abstract
Background: Intranasal vaccination may induce protective local and systemic immune responses against respiratory pathogens. A number of intranasal SARS-CoV-2 vaccine candidates have achieved protection in pre-clinical challenge models, including ChAdOx1 nCoV-19 (AZD1222, University of Oxford / AstraZeneca).
Methods: We performed a single-centre open-label Phase I clinical trial of intranasal vaccination with ChAdOx1 nCoV-19 in healthy adults, using the existing formulation produced for intramuscular administration. Thirty SARS-CoV-2 vaccine-naïve participants were allocated to receive 5 × 109 viral particles (VP, n=6), 2 × 1010 VP (n=12), or 5 × 1010 VP (n=12). Fourteen received second intranasal doses 28 days later. A further 12 received non-study intramuscular mRNA SARS-CoV-2 vaccination between study days 22 and 46. To investigate intranasal ChAdOx1 nCoV-19 as a booster, six participants who had previously received two intramuscular doses of ChAdOx1 nCoV-19 and six who had received two intramuscular doses of BNT162b2 (Pfizer / BioNTech) were given a single intranasal dose of 5 × 1010 VP of ChAdOx1 nCoV-19. Objectives were to assess safety (primary) and mucosal antibody responses (secondary).
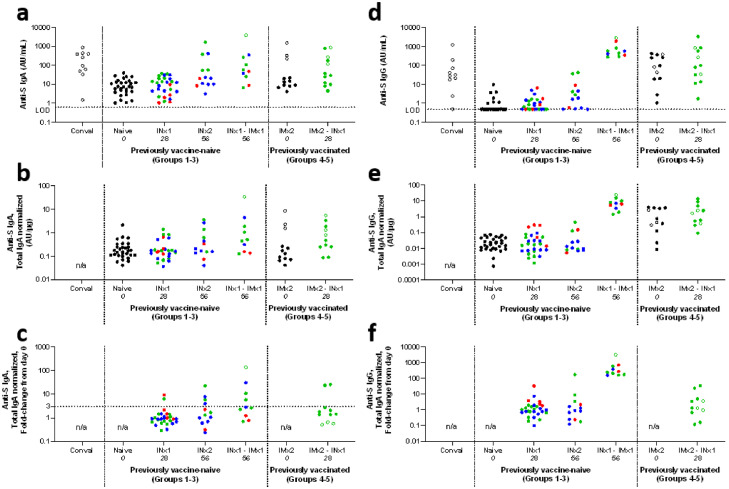
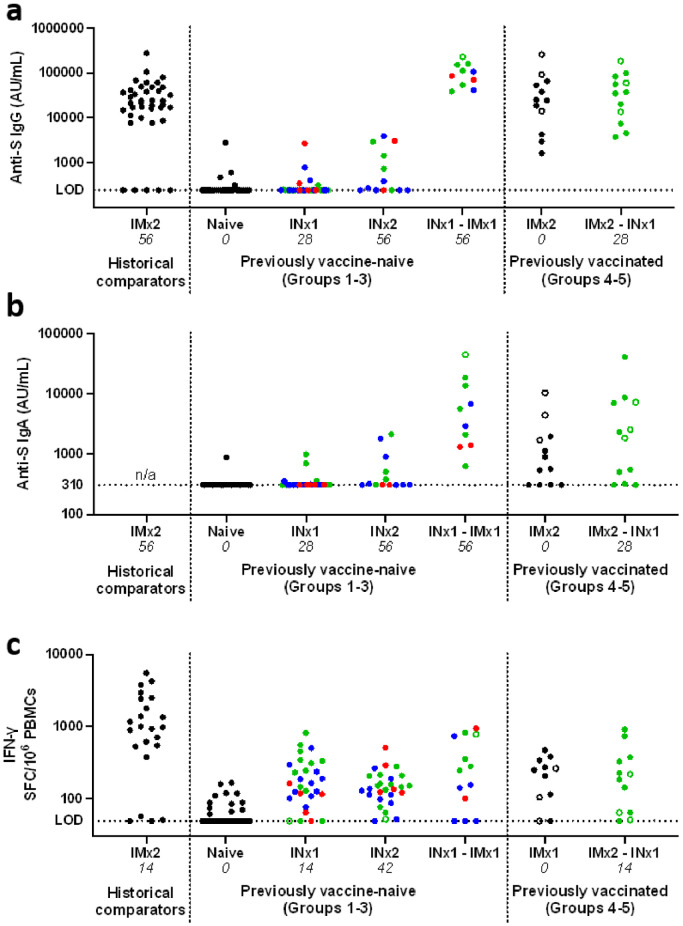
Findings: Reactogenicity was mild or moderate. Antigen-specific mucosal antibody responses to intranasal vaccination were detectable in a minority of participants, rarely exceeding levels seen after SARS-CoV-2 infection. Systemic responses to intranasal vaccination were typically weaker than after intramuscular vaccination with ChAdOx1 nCoV-19. Antigen-specific mucosal antibody was detectable in participants who received an intramuscular mRNA vaccine after intranasal vaccination. Seven participants developed symptomatic SARS-CoV-2 infection.
Interpretation: This formulation of intranasal ChAdOx1 nCoV-19 showed an acceptable tolerability profile but induced neither a consistent mucosal antibody response nor a strong systemic response.
Funding: AstraZeneca.
Keywords: Adenovirus vector; Intranasal vaccination; Mucosal antibody; SARS-CoV-2.
Copyright © 2022 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests Oxford University has entered into a partnership with AstraZeneca to develop ChAdOx1 nCoV-19. AJR and KE may receive royalties arising from the University of Oxford/AstraZeneca COVID-19 vaccine. TL is named as an inventor on a patent application covering this SARS-CoV-2 vaccine and was previously a consultant to Vaccitech on an unrelated project. AVSH is a cofounder of and former consultant to Vaccitech is named as an inventor on a patent covering design and use of ChAdOx1-vectored vaccines (PCT/GB2012/000467), and may receive royalties arising for the University of Oxford/AstraZeneca COVID-19 vaccine. DW, EJK, TV, and JAG are current employees of AstraZeneca and hold or may hold AstraZeneca stock. ADD reports grants and personal fees from AstraZeneca outside of the submitted work, is a named inventor on patent applications relating the chimpanzee adenovirus platform technology and manufacturing, and may receive royalties arising from the University of Oxford/AstraZeneca COVID-19 vaccine. All other authors declare no competing interests.
Figures


References
-
- Ponce-de-Leon S, Torres M, Soto-Ramirez LE, et al. Safety and immunogenicity of a live recombinant Newcastle disease virus-based COVID-19 vaccine (Patria) administered via the intramuscular or intranasal route: interim results of a non-randomized open label phase I trial in Mexico. medRxiv. 2022.
-
- Li JX, Wu SP, Guo XL, et al. Safety and immunogenicity of heterologous boost immunisation with an orally administered aerosolised Ad5-nCoV after two-dose priming with an inactivated SARS-CoV-2 vaccine in Chinese adults: a randomised, open-label, single-centre trial. Lancet Respir Med. 2022;10(8):739–748. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
