

Early dynamics of chronic myeloid leukemia on nilotinib predicts deep molecular response
- PMID: 36229495
- PMCID: PMC9561725
- DOI: 10.1038/s41540-022-00248-3
Early dynamics of chronic myeloid leukemia on nilotinib predicts deep molecular response
Abstract
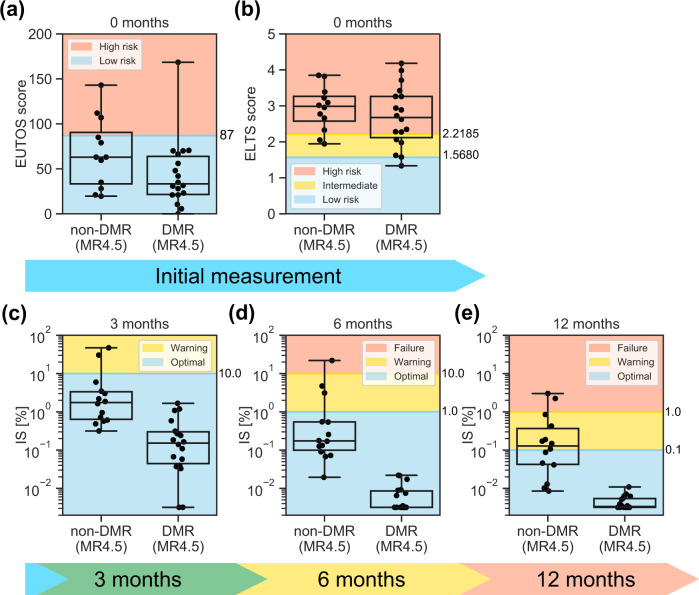
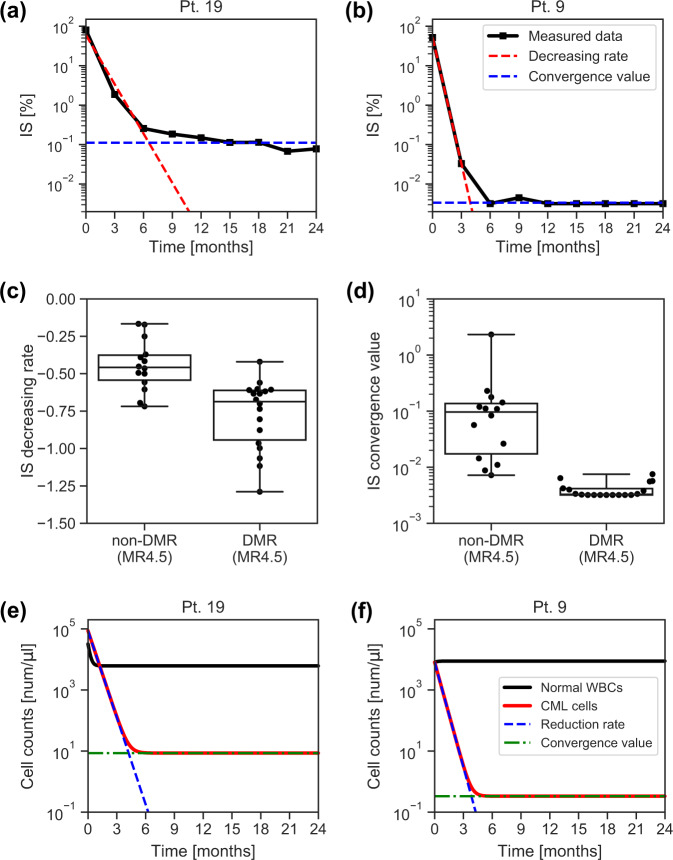
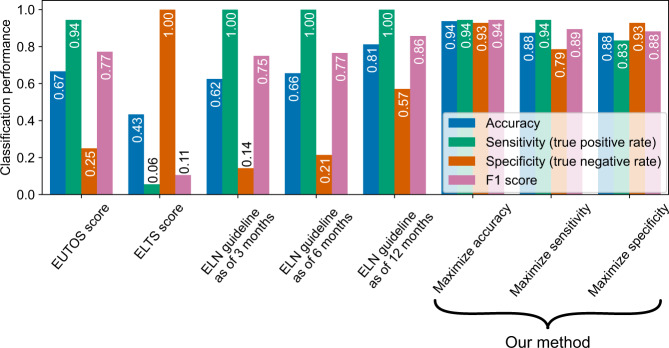
Chronic myeloid leukemia (CML) is a myeloproliferative disorder caused by the BCR-ABL1 tyrosine kinase. Although ABL1-specific tyrosine kinase inhibitors (TKIs) including nilotinib have dramatically improved the prognosis of patients with CML, the TKI efficacy depends on the individual patient. In this work, we found that the patients with different nilotinib responses can be classified by using the estimated parameters of our simple dynamical model with two common laboratory findings. Furthermore, our proposed method identified patients who failed to achieve a treatment goal with high fidelity according to the data collected only at three initial time points during nilotinib therapy. Since our model relies on the general properties of TKI response, our framework would be applicable to CML patients who receive frontline nilotinib or other TKIs.
© 2022. The Author(s).
Conflict of interest statement
K.M. reports a grant from NEC outside the submitted work. S.N. reports a grant from Morinaga Milk Industry Co., Ltd. outside the submitted work. K.N. received a grant for this work from Novartis Pharma K.K. and reports grants from Zenyaku Kogyo Company, Ltd., Asahi Kasei Pharma, and Taiho Pharmaceutical Co., Ltd.; grants and personal fees from Chugai Pharmaceutical, Kyowa Hakko Kirin Co., Ltd., Nippon Shinyaku Co., Ltd., Mochida Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., and Sumitomo Dainippon Pharma Co., Ltd.; and personal fees from Pfizer, Otsuka Pharmaceutical Co., Ltd., Janssen Pharmaceutical K.K., Eisai Co., Ltd., and Celgene K.K. outside of the submitted work. H.Y. reports grants from Celgene K.K. and Astellas Pharma Inc. outside the submitted work. A.T. reports personal fees from Sysmex, Otsuka Pharmaceutical Co., Ltd., Bristol-Myers Squib, and Takeda Pharmaceutical Co., Ltd., Daiichi-Sankyo and grants and personal fees from Pfizer, and Chugai Pharmaceutical outside the submitted work. K.A. reports a grant and personal fees from KKE, a grant and personal fees from NEC, a grant from Sysmex, a personal fee from Novo Nordisk Japan, and a grant and personal fees from Toyota Central R&D Labs. outside the submitted work. Y.O. had worked at Sysmex Co., but the entire results of this paper are totally independent from his past job in Sysmex Co.. The other authors have nothing to disclose.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
