

Clinical and molecular response to tebentafusp in previously treated patients with metastatic uveal melanoma: a phase 2 trial
- PMID: 36229663
- PMCID: PMC9671803
- DOI: 10.1038/s41591-022-02015-7
Clinical and molecular response to tebentafusp in previously treated patients with metastatic uveal melanoma: a phase 2 trial
Abstract
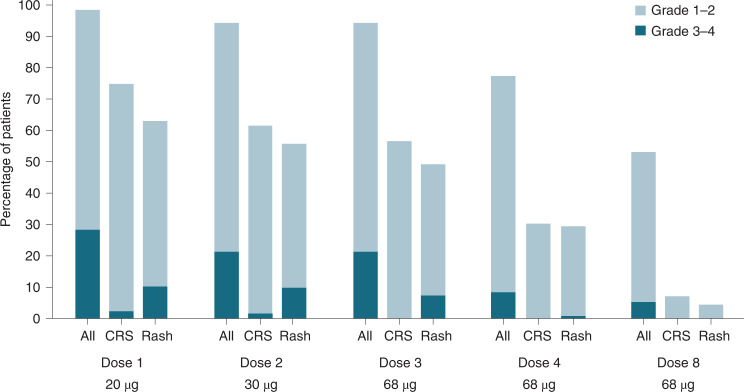
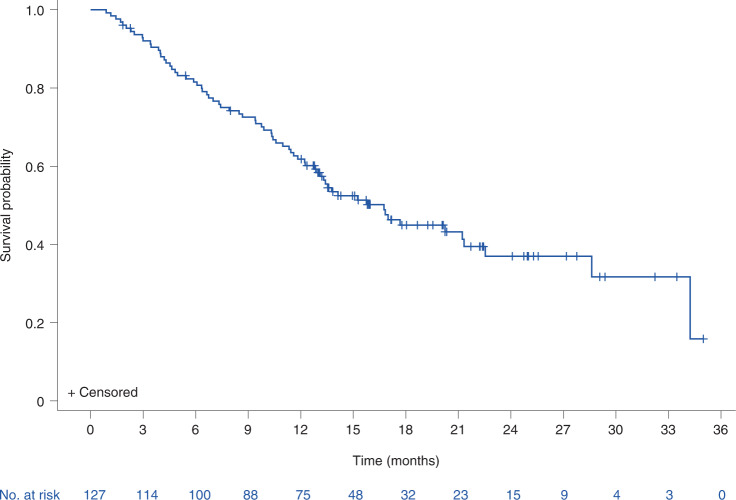
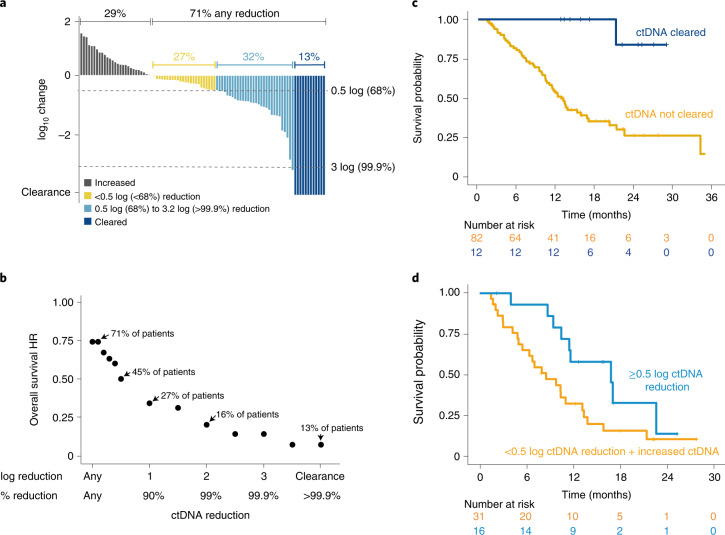
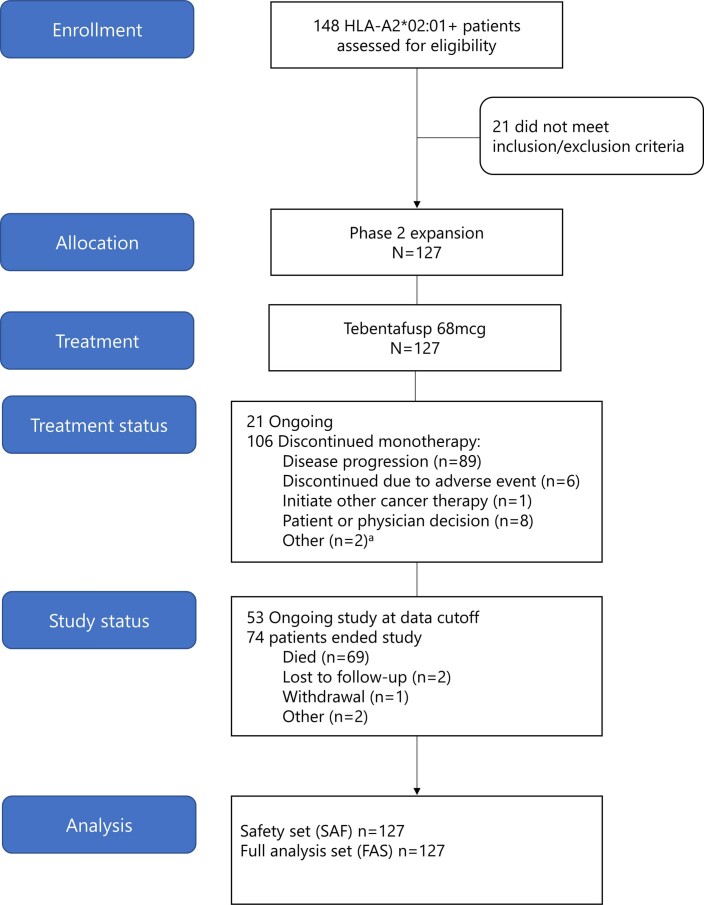
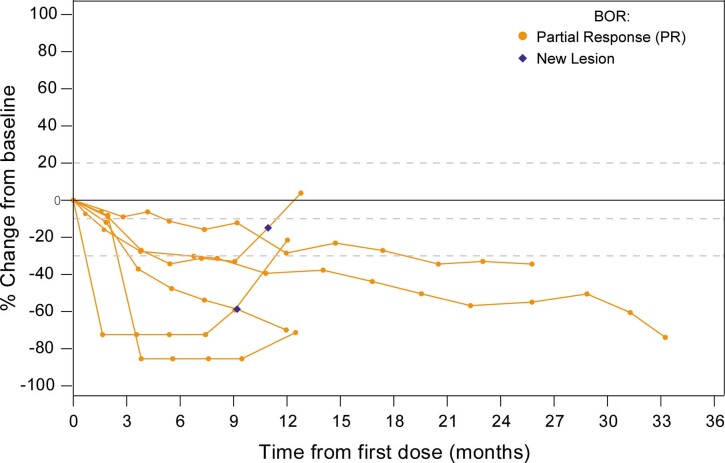
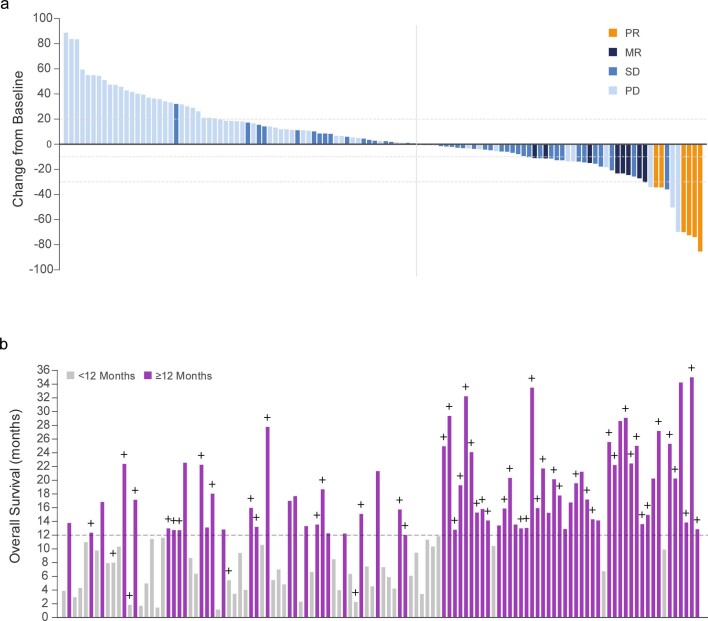
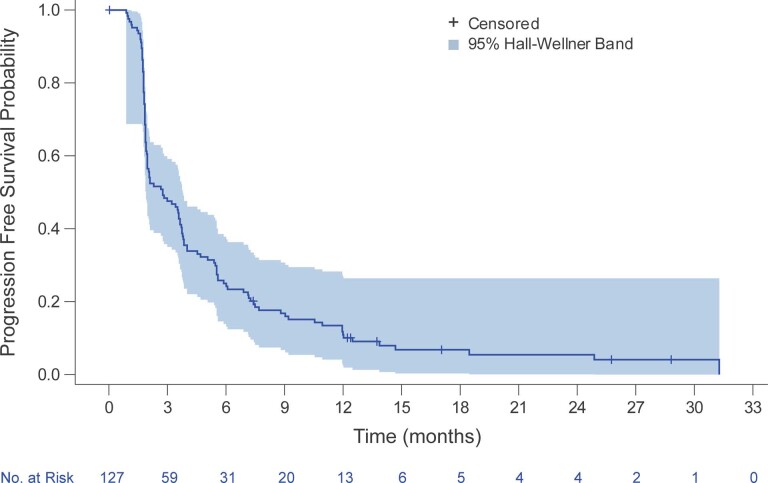
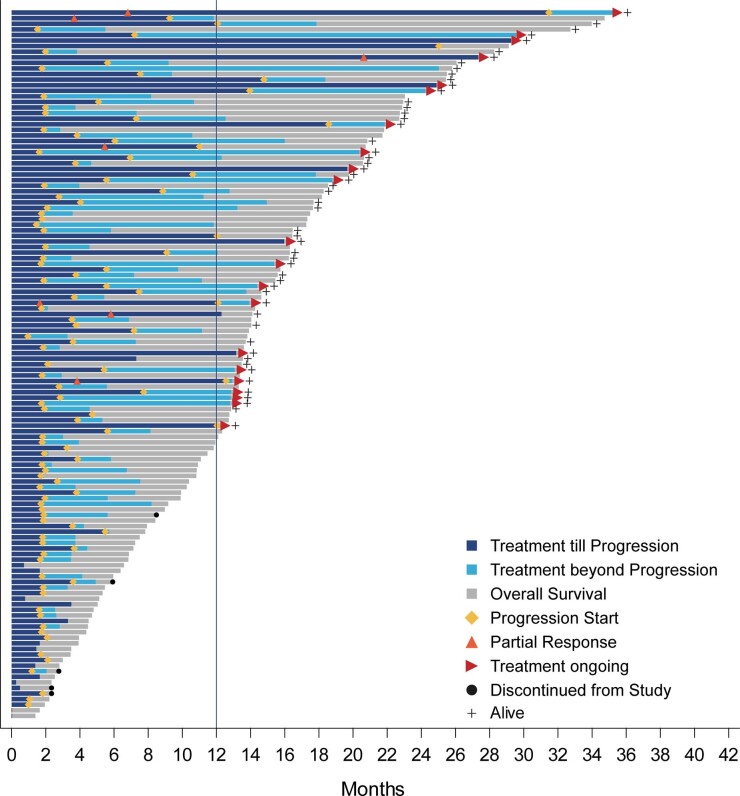
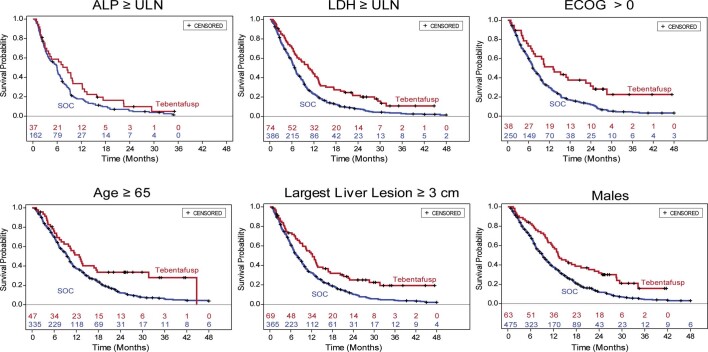
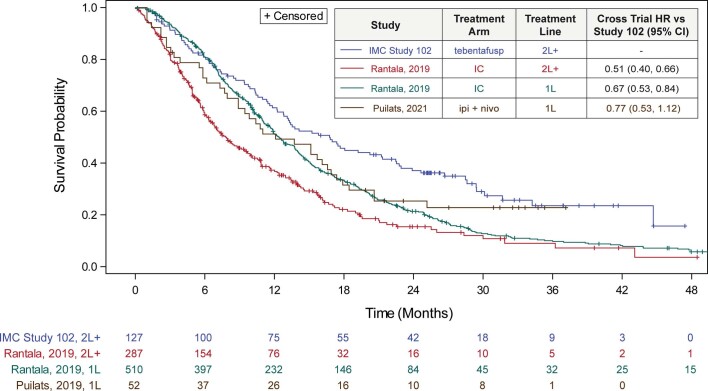
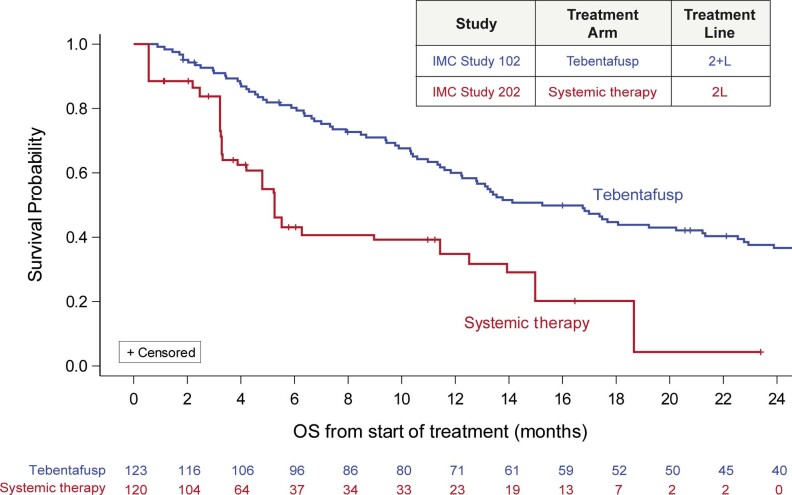
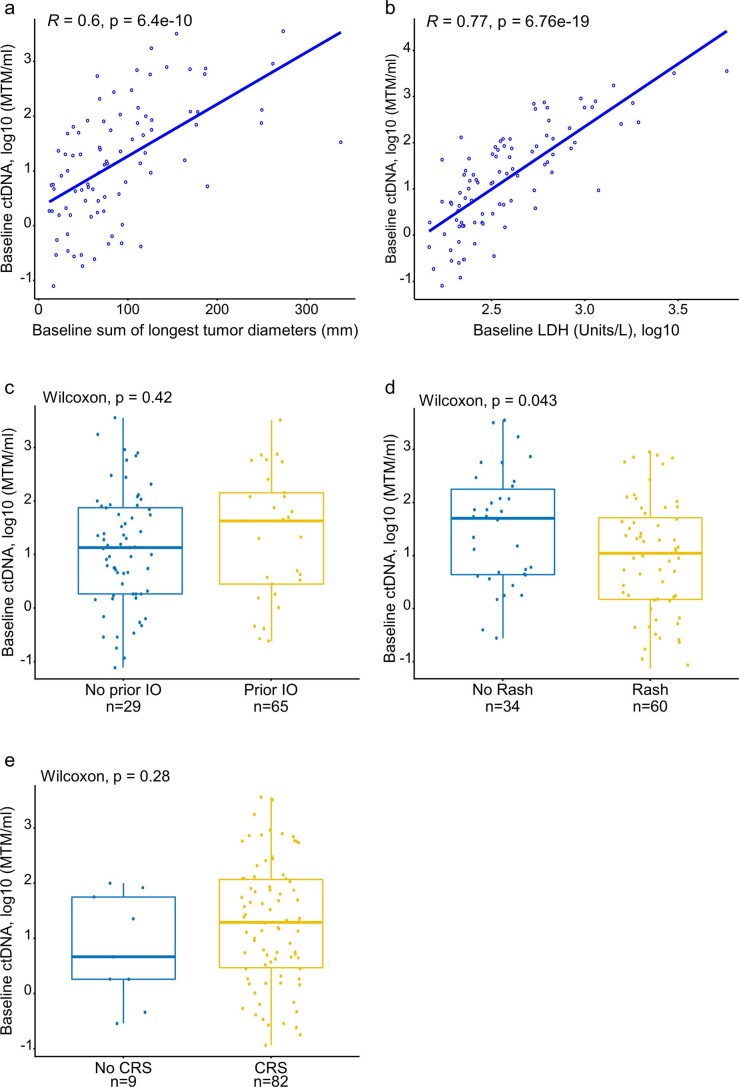
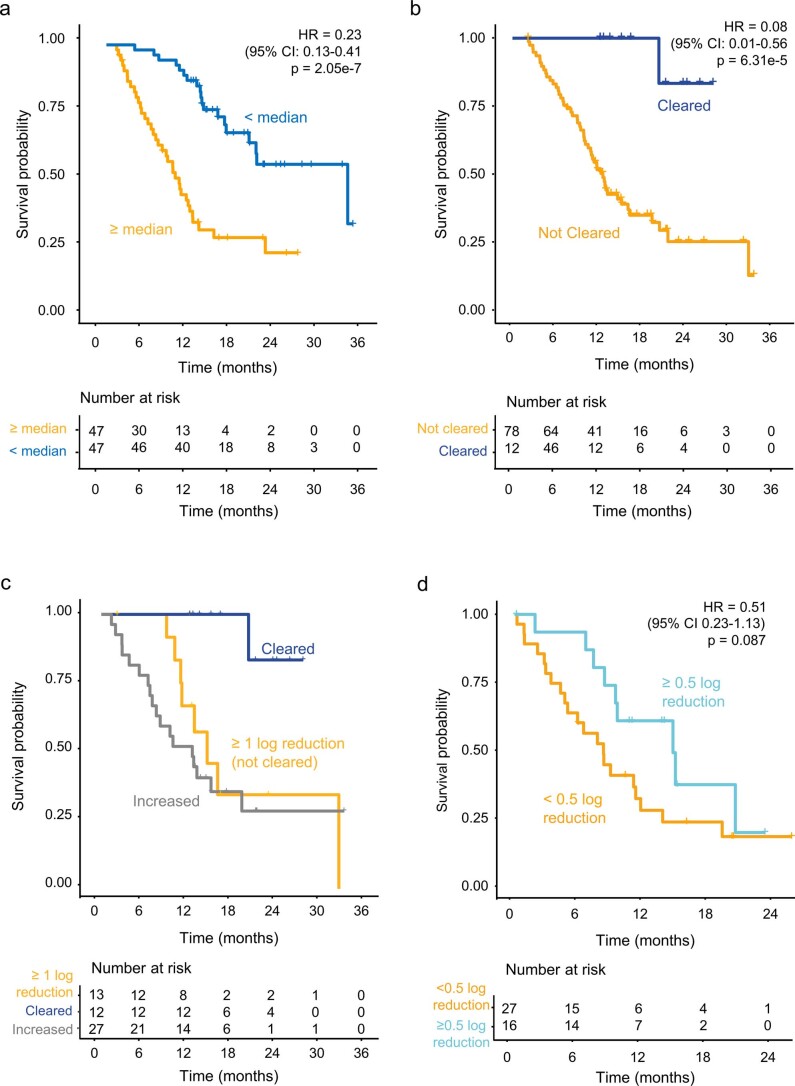
In patients with previously treated metastatic uveal melanoma, the historical 1 year overall survival rate is 37% with a median overall survival of 7.8 months. We conducted a multicenter, single-arm, open-label phase 2 study of tebentafusp, a soluble T cell receptor bispecific (gp100×CD3), in 127 patients with treatment-refractory metastatic uveal melanoma (NCT02570308). The primary endpoint was the estimation of objective response rate based on RECIST (Response Evaluation Criteria in Solid Tumours) v1.1. Secondary objectives included safety, overall survival, progression-free survival and disease control rate. All patients had at least one treatment-related adverse event, with rash (87%), pyrexia (80%) and pruritus (67%) being the most common. Toxicity was mostly mild to moderate in severity but was greatly reduced in incidence and intensity after the initial three doses. Despite a low overall response rate of 5% (95% CI: 2-10%), the 1 year overall survival rate was 62% (95% CI: 53-70%) with a median overall survival of 16.8 months (95% CI: 12.9-21.3), suggesting benefit beyond traditional radiographic-based response criteria. In an exploratory analysis, early on-treatment reduction in circulating tumour DNA was strongly associated with overall survival, even in patients with radiographic progression. Our findings indicate that tebentafusp has promising clinical activity with an acceptable safety profile in patients with previously treated metastatic uveal melanoma, and data suggesting ctDNA as an early indicator of clinical benefit from tebentafusp need confirmation in a randomized trial.
© 2022. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
R.D.C. discloses consulting: Alkermes, BMS, Castle Biosciences, Delcath, Eisai, Hengrui, Ideaya, Immunocore, InxMed, Iovance, Merck, Novartis, Oncosec, Pierre Fabre, PureTech Health, Regeneron, Sanofi Genzyme, Sorrento Therapeutics, Trisalus; clinical/scientific advisory boards: Aura Biosciences, Chimeron, Rgenix. M.O.B. discloses advisory/consulting: Merck, BMS, Novartis, Sanofi, Pfizer, Adaptimmune, GSK, Immunocore, EMD Serono, Sun Pharma, Medison, Instil Bio, IOVANCE; research funding to self: Merck, Takara Bio; research funding to institution: Merck, BMS, Novartis, Sanofi, Adaptimmune, Immunocore, Regeneron, Lilly, Amgen, OncoSeq; Speaker: BMS, Merck, Pfizer, Novartis, Sanofi. A.N.S. discloses honoraria advisory board/personal fees: BMS, Castle Biosciences, Immunocore, Novartis; licensing/royalties: UpToDate; research funding to institution: BMS, Checkmate Pharmaceuticals, Foghorn Therapeutics, GSK, Immunocore, Novartis, Pfizer, Polaris, Targovax, Xcovery. J.C.H. discloses advisory boards (self): GSK, MSD, Pierre Fabre, Sun Pharma; advisory boards (institution): BMS, Immunocore, Novartis, Nektar, Philogen; contracted research: 4SC, BioNTech, BMS, Genentech/Roche, Idera, Immunocore, Iovance, Nektar, Novartis, Philogen, Pierre Fabre, Regeneron, Sanofi; honoraria: BMS, MSD, Novartis, Pierre Fabre, Roche, Sanofi, Sun Pharma; research funding to institution: BMS, Sun Pharma. A.I. discloses research funding to institution: Checkmate Pharmaceuticals, Dynavax, GSK/Sarah Cannon, Immunocore, Merck, Neon Therapeutics/Sarah Cannon. L.H.-A. discloses advisory/consulting: BMS, Castle Bioscience; research funding to institution: BMS, AstraZeneca, Merck, Amgen, Roche, Regeneron, Novartis, Immunocore, Merck-EMD, Corvus, Polynoma, Genentech, Foghorn. P.N. discloses advisory/consulting: BMS, Immunocore, Ipsen, Incyte, MSD, Merck, Novartis, Pfizer, 4SC; speaker’s bureau: BMS, Merck, Novartis, Pfizer; research funding to institution: Immunocore, Novartis. O.H. discloses contracted research (institute): Aduro, Akeso, Amgen, Bioatla, BMS, Genentech, GSK, Idera, Immunocore, Incyte, Merck, NextCure, Novartis, Pfizer, Sanofi/Regeneron, SeaGen, Zelluna; speaker’s bureau: BMS, Novartis, Pfizer, Sanofi/Regeneron; consulting/advisory board: Aduro, Akeso, Amgen, Beigene, Bioatla, BMS, Genentech, GSK, Idera, Immunocore, Incyte, Janssen, Merck, NextCure, Novartis, Pfizer, Sanofi/Regeneron, SeaGen, Tempus, Zelluna. J.M.P. discloses research funding: BeiGene, BMS, Immunocore, Mirati, MSD. M.R. discloses consulting: Health Advances. D.B.J. discloses consultancy: BMS, Catalyst, Iovance, Janssen, Mallinckrodt, Merck, Mosaic, Novartis, Oncosec, Pfizer, Targovax, Teiko; non-remunerated activities: Melanoma Guideline Committee (NCCN), Scientific Selection Committee (ASCO), Immunotherapy Toxicity Guidelines (SITC); research funding to self: BMS, Incyte; research funding to institution: Array Biopharma, Genentech, Immunocore, Nektar. J.J.L. discloses consulting: Abbvie, Bayer, BMS, Castle, Checkmate, Codiak, Crown, Day One, Duke St, EMD Serono, Endeavor, Flame, Genentech, Gilead, Glenmark, HotSpot, Kadmon, Janssen, Ikena, Immunocore, Incyte, IO Biotech, Macrogenics, Merck, Nektar, Novartis, Partner, Pfizer, Regeneron, Roivant, Servier, STINGthera, Synlogic, Synthekine; scientific advisory board (no stock): 7 Hills, Bright Peak, Exo, Fstar, Inzen, RefleXion, Xilio; scientific advisory board (stock): Actym, Alphamab Oncology, Arch Oncology, Kanaph, Mavu, NeoTx, Onc.AI, OncoNano, Pyxis, STipe, Tempest; Data and Safety Monitoring Board: Abbvie, Immutep, Evaxion; research funding to institution: Abbvie, Astellas, AstraZeneca, BMS, Corvus, Day One, EMD Serono, Fstar, Genmab, Ikena, Immatics, Incyte, Kadmon, KAHR, Macrogenics. Merck, Moderna, Nektar, NextCure, Numab, Palleon, Pfizer, Replimmune, Rubius, Servier, Scholar Rock, Synlogic, Takeda, Trishula, Tizona, Xencor; patents (provisional): serial no. 15/612,657 (Cancer Immunotherapy), PCT/US18/36052 (Microbiome Biomarkers for Anti-PD-1/PD-L1 Responsiveness: Diagnostic, Prognostic and Therapeutic Uses Thereof). E.E. discloses consulting: BMS, MSD, Novartis, Pierre Fabre; non-remunerated activities: Vice-President (Grupo Espanol Melanoma); speaker bureau: BMS, MSD, Novartis, Pierre Fabre. S.L. discloses consulting: Bayer, Immunocore; expenses: Bayer. L.C., H.M.G., K.R., C.H. and S.E.A. are employees and have stocks/shares or stock options in Immunocore, which could benefit from commercialization of these results. J.J.S. discloses advisory/consulting: Immunocore, BMS, MSD, Delcath, Amgen; speaker’s bureau: BMS, MSD, Pierre Fabre; research funding to institution: Immunocore, BMS, MSD, Amgen, AstraZeneca, Replimune. T.S. discloses advisory/consulting: Immunocore, Castle Biosciences; research funding to institution: Immunocore, Verastem.
Figures
References
-
- Milam, R. W. & Daniels, A. B. Uveal melanoma. In Melanoma (ed. Riker, A.) pp. 273–312 (Springer, 2018). 10.1007/978-3-319-78310-9_16
-
- Stang A, Parkin DM, Ferlay J, Jöckel K. International uveal melanoma incidence trends in view of a decreasing proportion of morphological verification. Int. J. Cancer. 2005;114:114–123. - PubMed
-
- Virgili G, et al. Incidence of uveal melanoma in Europe. Ophthalmology. 2007;114:2309–2315. - PubMed
-
- Kujala E, Makitie T, Kivela T. Very long-term prognosis of patients with malignant uveal melanoma. Invest. Ophthalmol. Vis. Sci. 2003;44:4651–4659. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
