

Implementation of a standardized surgical technique in robot-assisted restorative rectal cancer resection: a single center cohort study
- PMID: 36229822
- PMCID: PMC9563459
- DOI: 10.1186/s12893-022-01809-3
Implementation of a standardized surgical technique in robot-assisted restorative rectal cancer resection: a single center cohort study
Abstract
Background: Despite increasing focus on the technical performance of total mesorectal excision over recent decades, anastomotic leakage (AL) continues to be a serious complication for many patients, even in the hands of experienced surgical teams. This study describes implementation of standardized surgical technique in an effort to reduce variability, decrease the risk of anastomotic leakage, and improve associated short-term outcomes for rectal cancer patients undergoing robot-assisted restorative rectal resection (RRR).
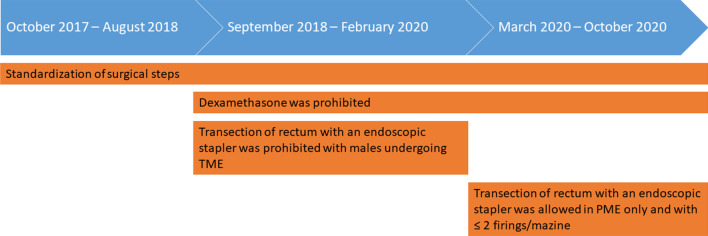
Methods: We evaluated all rectal cancer patients undergoing robot-assisted RRR at Aarhus University Hospital between 2017 and 2020. Six standardized surgical steps directed to improve anastomotic healing were mandatory for all RRR. Additional changes were made during the period with prohibition of systemic dexamethasone and limiting the use of endoscopic stapling devices.
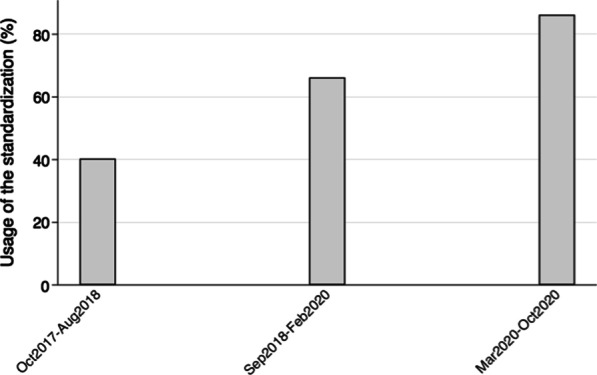
Results: The use of the full standardization, including all six surgical steps, increased from 40.3% (95% CI, 0.28-0.54) to 86.2% (95% CI, 0.68-0.95). The incidence of AL decreased from 21.0% (95% CI, 0.12-0.33) to 6.9% (95% CI, 0.01-0.23). Length of hospital stay (LOS) decreased from 6 days (range 2-50) to 5 days (range 2-26). The rate of patients readmitted within 90 days decreased from 21.0% (95% CI, 0.12-0.33), to 6.9% (95% CI, 0.01-0.23).
Conclusion: The full standardization was effectively implemented for rectal cancer patients undergoing robot-assisted RRR. The risk of AL, LOS and readmission decreased during the study period. A team focus on high-reliability and peri-operative complications can improve patient outcomes.
Keywords: Anastomotic leakage; Implementation; Rectal cancer; Robot; Standardization; Surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Cancer Today [Internet]. Available from: https://gco.iarc.fr/today/home (Accessed: 19 October 2021).
-
- Schnitzbauer V, Gerken M, Benz S, Völkel V, Draeger T, Fürst A, et al. Laparoscopic and open surgery in rectal cancer patients in Germany: short and long-term results of a large 10-year population-based cohort. Surg Endosc [Internet]. 2020;34(3):1132–1141. doi: 10.1007/s00464-019-06861-4. - DOI - PMC - PubMed
-
- Fleshman J, Branda ME, Sargent DJ, Boller AM, George VV, Abbas MA, et al. Disease-free survival and local recurrence for laparoscopic resection compared with open resection of stage II to III rectal cancer: follow-up results of the ACOSOG Z6051 randomized controlled trial. Ann Surg. 2019;269(4):589–595. doi: 10.1097/SLA.0000000000003002. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
