

Management after initial surgery of nonfunctioning pituitary adenoma: surveillance, radiotherapy or surgery?
- PMID: 36229880
- PMCID: PMC9559766
- DOI: 10.1186/s13014-022-02133-z
Management after initial surgery of nonfunctioning pituitary adenoma: surveillance, radiotherapy or surgery?
Abstract
Introduction: The first line of treatment for nonfunctioning pituitary adenoma (NFPA) is surgery. Adjuvant radiotherapy or surveillance and new treatment (second surgical operation or salvage radiotherapy) in case of recurrence are options discussed at the multidisciplinary tumor board. The purpose of this study was to evaluate the therapeutic outcome for each option.
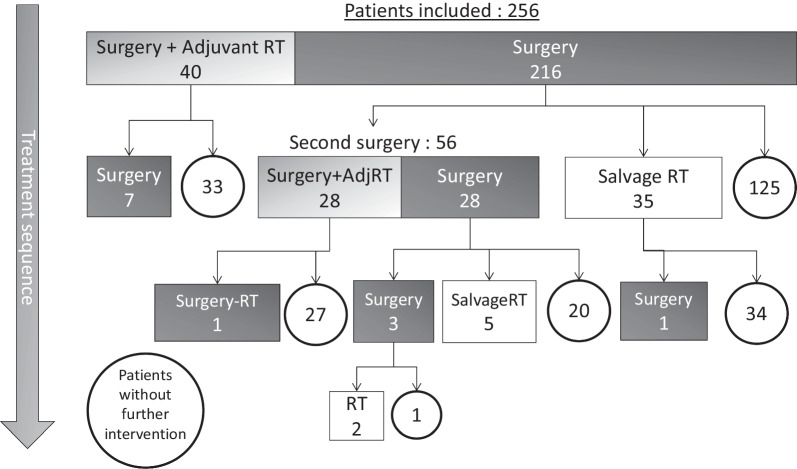
Methods: The records of 256 patients followed with NFPA between 2007 and 2018 were retrospectively reviewed. Mean age at initial surgery was 55 years [18-86]. Post-operative MRI found a residual tumor in 87% of patients. Mean follow-up was 12.1 years [0.8-42.7].
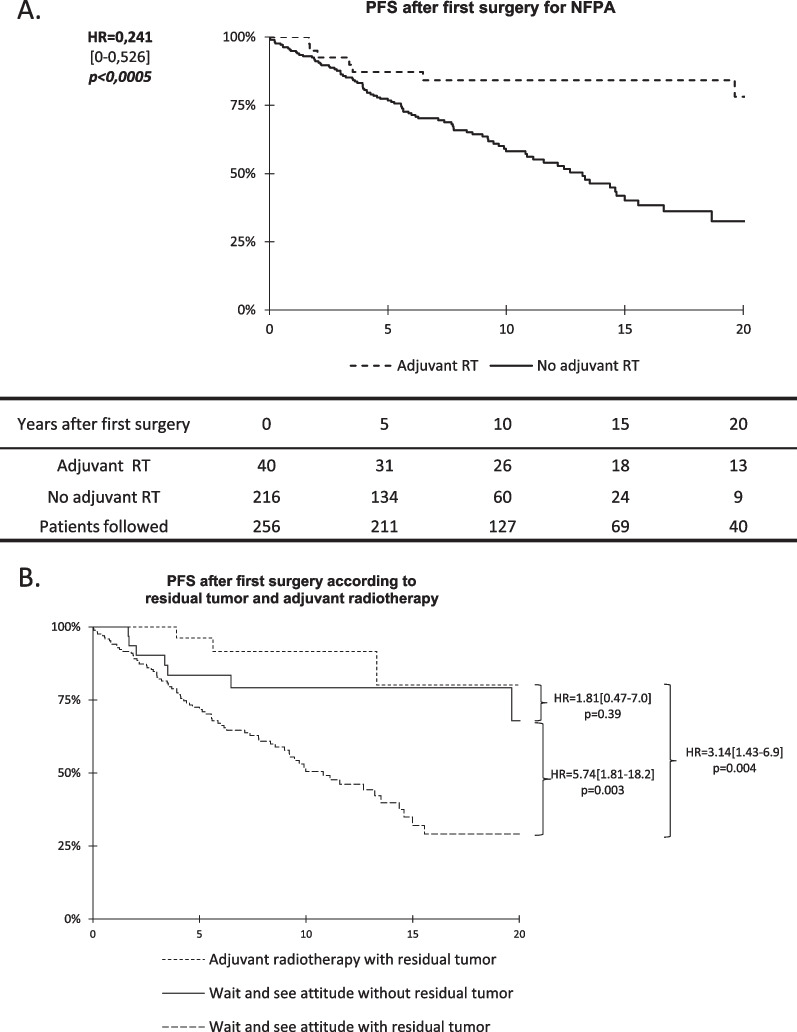
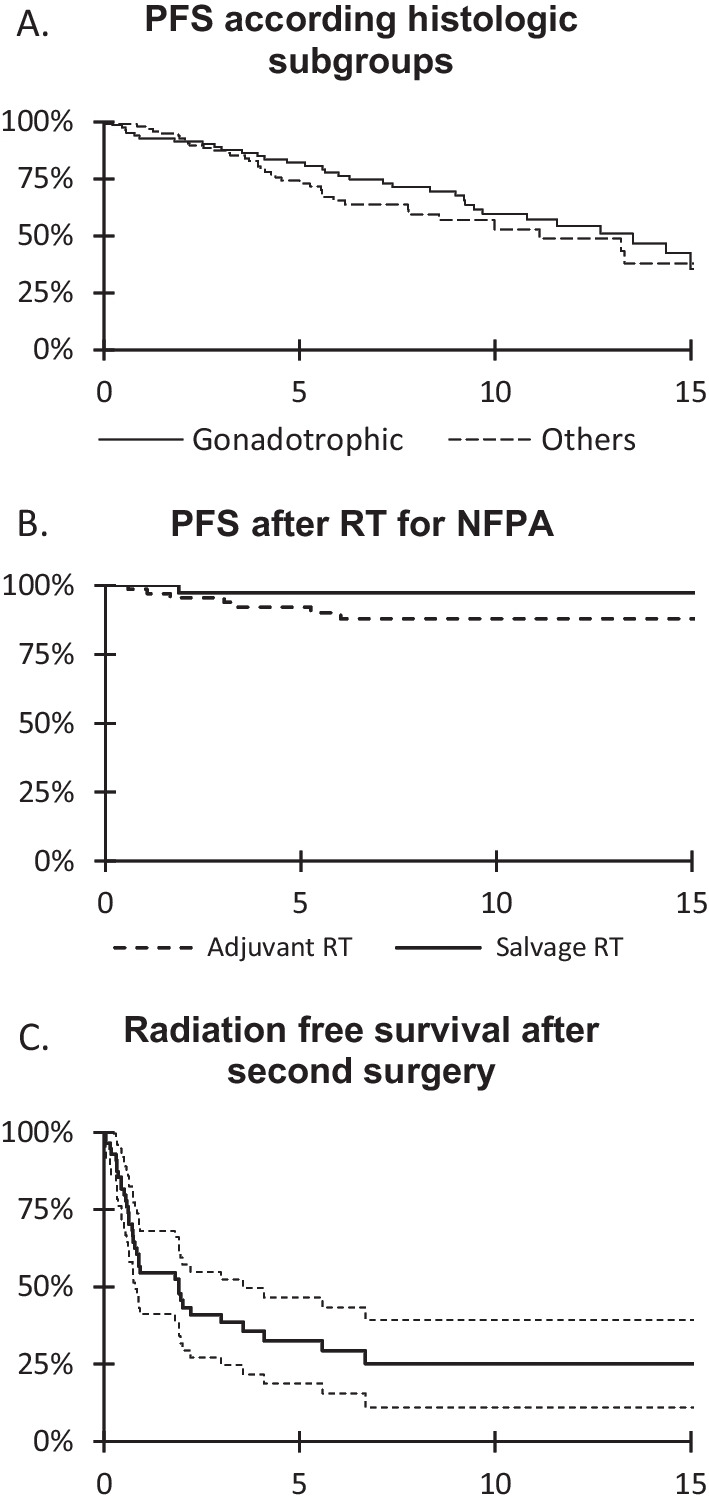
Results: After initial surgery, 40 patients had adjuvant radiotherapy. At 5, 10 and 15 years progression-free survival (PFS) was significantly different after surgery alone (77%, 58% and 40%) compared to surgery and adjuvant radiotherapy (84%, 78% and 78%) (HR = 0.24 [0-0.53] p < 0.0005). Overall, after first, second or third surgical operation, 69 patients had adjuvant radiotherapy and 41 salvage radiotherapy. Five-year PFS was similar for adjuvant (90%) and salvage radiotherapy (97%) (p = 0.62). After a second surgical operation, 62% and 71% of patients were irradiated after 2 and 5 years respectively. The risk of corticotropic and thyrotropic deficiency rates were 38% and 59% after second or third surgical operation and 40% and 73% after radiotherapy. Brain tumors occurred in 4 patients: 1 meningioma present at initial surgery, and after radiotherapy, 1 neurinoma which appeared at 5 years, 1 glioblastoma at 13 years and 1 meningioma at 20 years.
Conclusion: Among patients treated by surgery for NFPA, a "wait-and-see" attitude should be an option since adjuvant radiotherapy is not superior to salvage radiotherapy. However, in case of recurrence or progression, the authors recommended delivery of salvage radiotherapy to avoid a second surgical operation.
Keywords: Non-functioning pituitary adenoma; Radiotherapy; Surgery; Wait and see.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Loiseau H, Huchet A, Baldi I. Épidémiologie des tumeurs cérébrales primitives. Neurologie.com. 2010;4:83–6. - PubMed
-
- Lucas JW, Bodach ME, Tumialan LM, Oyesiku NM, Patil CG, Litvack Z, et al. Congress of neurological surgeons systematic review and evidence-based guideline on primary management of patients with nonfunctioning pituitary adenomas. Neurosurgery. 2016;79(4):E533–535. doi: 10.1227/NEU.0000000000001389. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
