

Evaluation of a fast-and-frugal clinical decision algorithm ('pathways') on clinical outcomes in hospitalised patients with COVID-19 treated with anticoagulants
- PMID: 36229950
- PMCID: PMC9840687
- DOI: 10.1111/jep.13780
Evaluation of a fast-and-frugal clinical decision algorithm ('pathways') on clinical outcomes in hospitalised patients with COVID-19 treated with anticoagulants
Abstract
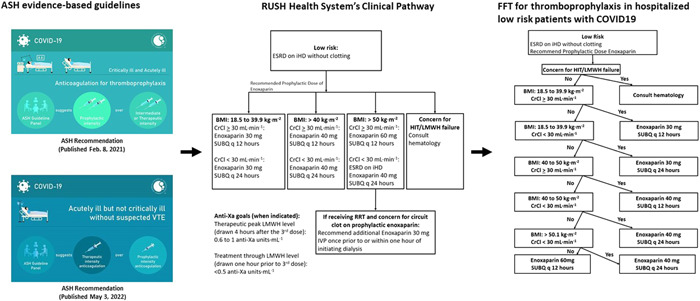
Rationale, aims and objectives: Critics have charged that evidence-based medicine (EBM) overemphasises algorithmic rules over unstructured clinical experience and intuition, but the role of structured decision support systems in improving health outcomes remains uncertain. We aim to assess if delivery of anticoagulant prophylaxis in hospitalised patients with COVID-19 according to an algorithm based on evidence-based clinical practice guideline (CPG) improved clinical outcomes compared with administration of anticoagulant treatment given at individual practitioners' discretion.
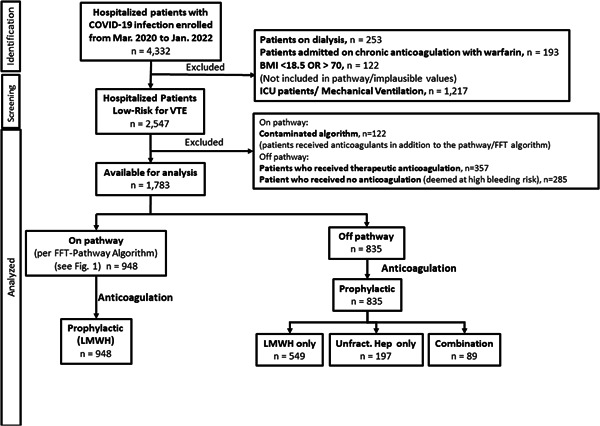
Methods: An observational design consisting of the analysis of all acutely ill, consecutive patients (n = 1783) with confirmed COVID-19 diagnosis admitted between 10 March 2020 to 11 January 2022 to an US academic center. American Society of Haematology CPG for anticoagulant prophylaxis in hospitalised patients with COVID-19 was converted into a clinical pathway and translated into fast-and-frugal decision (FFT) tree ('algorithm'). We compared delivery of anticoagulant prophylaxis in hospitalised patients with COVID-19 according to the FFT algorithm with administration of anticoagulant treatment given at individual practitioners' discretion.
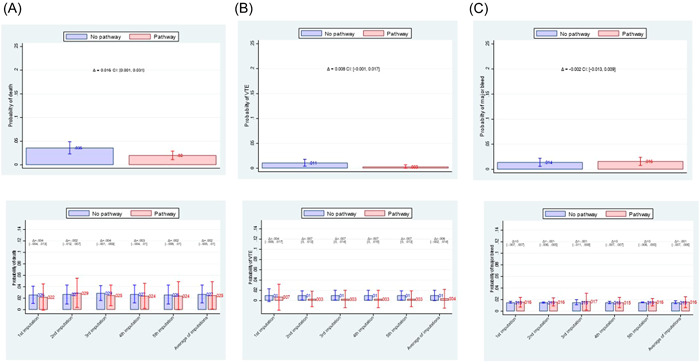
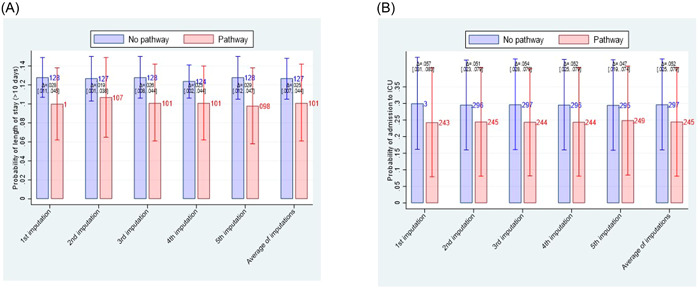
Results: In an adjusted analysis, using combination of Lasso (least absolute shrinkage and selection operator) and propensity score based weighting [augmented inverse-probability weighting] statistical techniques controlling for cluster data, the algorithm did not reduce death, venous thromboembolism, or major bleeding, but helped avoid longer hospital stay [number of patients needed to be treated (NNT) = 40 (95% CI: 23-143), indicating that for every 40 patients (23-143) managed on FFT algorithm, one avoided staying in hospital longer than 10 days] and averted admission to intensive-care unit (ICU) [NNT = 19 (95% CI: 13-40)]. All model's selected covariates were well balanced. The results remained robust to sensitivity analyses used to test the stability of the findings.
Conclusions: When delivered using a structured FFT algorithm, CPG shortened the hospital stay and help avoided admission to ICU, but it did not affect other relevant outcomes.
Keywords: clinical decision making; clinical pathways; decision support; evidence based medicine; fast-and-frugal trees; practice guidelines.
© 2022 The Authors. Journal of Evaluation in Clinical Practice published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Djulbegovic B, Guyatt GH. Progress in evidence‐based medicine: a quarter century on. Lancet. 2017;390(10092):415‐423. - PubMed
-
- Graham R, Mancher M, Wolman DM, Greenfield S, Steinberg E, Editors., Clinical Practice Guidelines we can Trust.Institute of Medicine, National Academies Press; 2011. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
